Understanding the configuration of the root canal systems in detail improves the success rates of root canal treatment and long-term prognosis. A cross-sectional was conducted to evaluate the root canal variations in the mandibular premolar teeth. 151 mandibular premolar teeth were analyzed using cone-beam computed tomographic scans. The pulp canal configuration of first mandibular premolar and second mandibular premolar were analyzed using axial, coronal, and sagittal sections. The results revealed that 89.4 % of the examined teeth were found to have more than one canal at the apical one-third and 10.6% had one root canal. Vertucci’s type V root canal morphology was the most frequent morphological type in both the first and second premolars (50.3%). The next prevalent types were type I (10.6%) and type III (9.3%). The prevalence of other types that were not defined in Vertucci’s classification was 11.3%. It was concluded that the most common root canal configurations in the present study were Type V followed by Type I. The study highlights the importance of variations in root canal morphology of mandibular premolars. There is a need for the reclassification of root canal systems using advanced three-dimensional cone beam computed tomographic imaging.
Introduction
What does it take to perform a successful endodontic treatment? Certainly, complete eradication of infection source followed by adequate root/pulp canal sealing. Root canal morphology plays a key role in successful root canal therapy [1]. Failure to identify the variations in the root canal can result in post-endodontic treatment complications or failure.
Endodontic treatment failure is mostly attributed to a microbial etiology or the inability to locate or access root canals. Incomplete biomechanical preparations or root canal filling can also contribute to the failure. However, persistent infection or secondary infection of the root canal contributes to be predominant factor in endodontic treatment failures [2]. Posterior teeth have the highest endodontic failures in comparison to the anterior teeth owing to differences in the pulp canal configuration and the failure of the dental practitioner to detect and access accessory or lateral canals or due to procedural errors [3]. The classification of root canal morphology by Vertucci was primarily based on two-dimensional (2D) data [4, 5]. As technology advanced, the incorporation of cone-beam computed tomography (CBCT) in endodontics changed the way advanced endodontics had been practiced. CBCT in endodontics helps in 3D visualization of the root canal morphology, providing fine details comparable to MDCT, but with reduced radiation dose and cost [6].
Analysis of morphological variations in canal configurations using 3D CBCT becomes inevitable to perform a detailed evaluation of the root canal morphology, especially in cases of post-endodontic treatment complications or failures. It is important to validate whether any variation exists in root canal morphology classification detailed in the scientific literature based on Vertucci’s classification using 2D imaging in comparison to the data retrieved from 3D CBCT of the root canal morphology for mandibular premolars. There are multiple studies in different geographical niches evaluating the root canal morphology using CBCT, mainly of posterior teeth [6-8]. Since ethnicity can influence the variation in root canal morphology and there is a scarcity of studies in Saudi Arabia that focus on both first and second mandibular premolar root canal morphological variations using CBCT, there is a need to analyze and comprehend this data. The outcomes of this study will aid dental practitioners in successfully performing endodontic treatment, especially in assessed cases where endodontic therapy failures are encountered resulting in post-endodontic complications.
Hence, our study aimed to investigate the root canal configurations of mandibular premolars by means of cone beam computed tomography imaging.
Materials and Methods
The manuscript was prepared in adherence to Preferred Reporting of Observational Studies in Endodontics (PROBE) guidelines.
A retrospective cross-sectional observational study was performed using CBCT scans of 151 cases retrieved from scans captured using Sirona Galileos (Germany) at 85 kV, 5 -7 mA, and 14s, from the Radiology Section of Private Dental University (affiliated to the University of the investigators). Analysis was done using Galileos viewer (version 1.9, Germany). Data collection and processing were done in adherence to the declaration of Helsinki (2013) after Ethical committee approval (RC/IRB/2019/308). Data screening was done from 2018 to 2023 and the inclusion/exclusion criteria were applied to collect the data to be included in the study.
The inclusion criteria were as follows: Age range from 16 to 60 years, full view of one or more mandibular premolars, complete root formation, no sign of root resorption, no periapical lesion, and no endodontic treatment, posts or coronal restorations, images with errors. Exclusion criteria were CBCT images with artifacts or errors, white streaking, and beam hardening in CBCT images which compromises the accuracy of the data, pathologies, or fracture/ endodontically treated tooth. Personal data will not be included in this study.
Methodology
CBCT scans were scrutinized for the root canal configuration using Galileo’s CBCT viewer (version 1.9) with a resolution of 286um. 3D digital imaging system by an Oral and Maxillofacial Radiologist using Vertucci 1994 classification. Hence no interobserver bias was recorded. Each reading was taken thrice and the average was taken as the final value of the observation to avoid intraobserver bias.
The evaluation was done in axial and coronal cross-section views using multi-planar reformatted images. The root canal was evaluated from the CEJ along the long axis of the tooth and viewed in axial sections from its start along its path to the apical foramen. All scans were analyzed by an Oral and Maxillofacial Radiologist with more than 9 years of experience in reading CBCT images. The co-investigator contributed to analyzing the data for statistical inference.
Inclusion criteria for the study were CBCT images of mandibular first and second premolars, Saudi population, CBCT images of diagnostic quality, and SAe 16 to 60 years. Exclusion criteria applied were data from the non-Saudi population, errors or artifacts in the region of interest in the CBCT images, implants in the area of interest, periapical pathology, and endodontically treated teeth.
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) version 26.0 (SPSS Inc., Chicago, IL, USA). Frequencies and percentages were used for data description. A chi-square test for independence and Fisher's exact test was used to assess the differences between groups in terms of the distribution of Vertucci’s morphological types. A p-value of < 0.05 was considered statistically significant.
Results and Discussion
In the present study, mandibular premolars were examined for root canal morphology according to Vertucci’s classification using cone beam computed tomography (CBCT). 270 CBCT scans were screened from the period of 2018 to 2023. Data of the patients was filtered by applying the inclusion and exclusion criteria. 45 premolars were excluded due to Root canal treatment (RCT), 37 premolars were absent; 4 were Implants; 2 teeth with periapical pathologies 8 CBCT images had artifacts/errors in the region of interest and 7 were completely edentulous. 16 patients were excluded due to being Non- Saudis and 22 patients were under 16 years or over 60 years (to ensure complete root formation and on the other hand to exclude the age-related changes in the pulp canal which can affect the results of the study). Thus, a total of 151 teeth were included in the analysis.
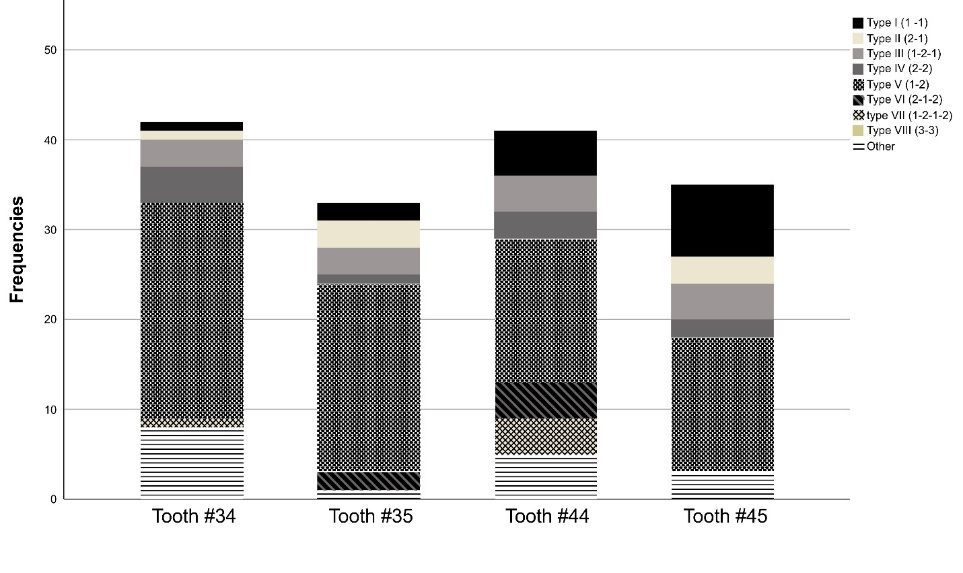
Males represented more than half of the study sample (56.0%), and the most predominant age group was 31 to 45 years of age (46.0%) (Table 1). The mandibular first premolars represented 55.0% of the study sample. It was noted that 89.4 % of the examined teeth had more than one canal and 10.6% had one root canal. Vertucci’s type V configuration of root canal morphology was the most frequently revealed morphological type among all canal types in both the premolars (50.3%), followed by type I (10.6%) and type III (9.3%) (Figure 1). The prevalence of other types that were not defined in Vertucci’s classification was 11.3% (Figure 2).
Table 1. Demographic characteristics of patients (n=50) and the distribution of Vertucci classification in premolar teeth (n=151)
|
Parameter |
Category |
Frequency |
Percentage |
|
Gender |
Male |
28 |
56.0 |
|
Female |
22 |
44.0 |
|
|
Age group |
16 to 30 y |
16 |
32.0 |
|
31 to 45 y |
23 |
46.0 |
|
|
46 to 60 y |
11 |
22.0 |
|
|
Premolars* |
First premolar |
83 |
55.0 |
|
Second premolar |
68 |
45.0 |
|
|
Vertucci Classification* |
Type I (1 -1) |
16 |
10.6 |
|
Type II (2-1) |
7 |
4.6 |
|
|
Type III (1-2-1) |
14 |
9.3 |
|
|
Type IV (2-2) |
10 |
6.6 |
|
|
Type V (1-2) |
76 |
50.3 |
|
|
Type VI (2-1-2) |
6 |
4.0 |
|
|
type VII (1-2-1-2) |
5 |
3.3 |
|
|
Type VIII (3-3) |
0 |
0.0 |
|
|
Other types |
17 |
11.3 |
|
|
|
Figure 1. The distribution of different Vertucci’s morphological types in mandibular premolars. |
|
|
|
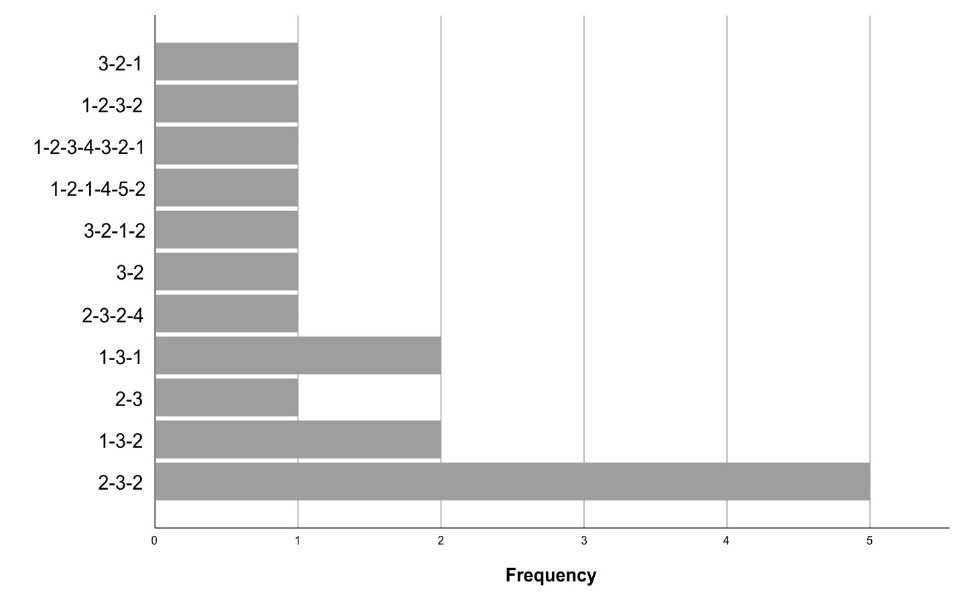
Figure 2. The frequencies of ‘other’ types of root canal morphologies in mandibular premolar |
The root canal configuration exhibited gender difference, where males had significantly higher proportions of type II configuration (6.9% vs 1.6%) and other types of vertucci’s canal configuration compared to females (14.9% vs 6.3%, p = 0.016) as depicted in Table 2. Furthermore, there were significant differences between first and second premolars in terms of their root canal configuration. Type I and II canals were significantly lower in the mandibular first premolars in comparison to the mandibular second premolar (7.2% vs 14.7% and 1.2% vs 8.8%, respectively), whereas other types of vertucci’s canal configuration were more prevalent in first premolar teeth (15.7% vs 5.9%, p = 0.030). Among the ‘other types,’ canal configuration was 1-3-1, and 1-3-2 had equal preponderance. However, root canal configuration did not differ according to the age of the study population (Table 2).
Table 2. Distribution of Vertucci classification in premolar teeth according to gender, age, and tooth location
|
Parameter |
Category |
Vertucci’s classification n (%) |
p |
|||||||
|
Type I |
Type II |
Type III |
Type IV |
Type V |
Type VI |
Type VII |
Other |
|||
|
Gender |
Male |
10 (11.5) |
6 (6.9) |
8 (9.2) |
10 (11.5) |
35 (40.2) |
3 (3.4) |
2 (2.3) |
13 (14.9) |
0.016 |
|
Female |
6 (9.4) |
1 (1.6) |
6 (9.4) |
0 (0.0) |
41 (64.1) |
3 (4.7) |
3 (4.7) |
4 (6.3) |
||
|
Age group |
16 to 30 y |
3 (6.1) |
3 (6.1) |
3 (6.1) |
3 (6.1) |
31 (63.3) |
1 (2.0) |
1 (2.0) |
4 (8.2) |
0.207 |
|
31 to 45 y |
8 (11.4) |
1 (1.4) |
8 (11.4) |
5 (7.1) |
28 (40.0) |
4 (5.7) |
3 (4.3) |
13 (18.6) |
||
|
46 to 60 y |
5 (15.6) |
3 (9.4) |
3 (9.4) |
2 (6.3) |
17 (53.1) |
1 (3.1) |
1 (3.1) |
0 (0.0) |
||
|
Premolars |
First Premolar |
6 (7.2) |
1 (1.2) |
7 (8.4) |
7 (8.4) |
40 (48.2) |
4 (4.8) |
5 (6.0) |
13 (15.7) |
0.030 |
|
Second Premolar |
10 (14.7) |
6 (8.8) |
7 (10.3) |
3 (4.4) |
36 (52.9) |
2 (2.9) |
0 (0.0) |
4 (5.9) |
||
The level of division of the root canal in single bifurcated root canal morphological types (which divided only one time from the starting of the root canal at the region of CEJ along its path to apical foramen) such as in Type III (1-2-1), Type IV(2-2), Type V (1-2), Type VI (2-1-2) were scrutinized and detected in 87 teeth among the 151 teeth evaluated. Type V was the most predominant teeth (80.5%) with single root canal bifurcation, followed by Type II(9.2%), type IV (8%), Type IV(1.15%), and another type (1.15%). The level of division in these single bifurcated root canal morphological types was more common at the middle 1/3rd root region (64.4%), followed by apical 1/3rd root region (23%) and cervical 1/3rd root region (12.6%). Type V single root canal bifurcation (70 teeth out of 87 teeth) occurred mostly at the middle 1/3rd of the root in 41 teeth(58.6%), followed by apical 1/3rd in 18 teeth (25.7%), and the root canal bifurcation at the cervical 1/3rd of the tooth was the least seen as in 11 teeth (15.7%). There is an increased prevalence of multiple canals in the mandibular premolars.
The present study evaluated the root canal morphological variations in mandibular premolars in the subpopulation of Saudi Arabia. This observational study re-iterates the advantages of 3D imaging in obtaining minute anatomical or morphological details that often remain obscured in 2D radiographic imaging.
The present study observed a higher prevalence of Type V root canal morphological type in mandibular premolars. Also, another remarkable finding was the prevalence of more than one canal in mandibular premolars (89.4%). The finding of this study correlates with the observations of a Micro CT study conducted in Brazil which noted that 58.57% of mandibular first premolars had a type V root canal configuration [7, 9, 10]. The 3D models of the mandibular premolars in this study give us a visual glimpse of the minute findings that can be recorded with 3D imaging. Our results were similar to a recent systematic review and meta-analysis performed for mandibular premolar root canal configuration using CBCT. In this systematic review and metal analysis, type V was the most common root canal configuration reported followed by type IV, type III, and type IV respectively [11]. It has to be noted that there is a higher prevalence of Type V canals detected using CBCT than observed from previous studies [7, 12-15].
The results of the present study are comparable to the study in Caucasians among 400 dark-skinned and 400 white-skinned mandibular premolars, in which more than one root canal in the mandibular first premolars was more common in dark-skinned people than the whites and also more than one canal was significantly found in at least one premolar in dark-skinned people than the whites (39% vs 13.7%) [16, 17]. In another study, more than two or three root canals were observed in 23.1% of first mandibular premolars and 12.1% in second mandibular premolars out of 2331 premolars by radiographic and mechanical probing [18, 19]. Though these studies analyzed 2D radiographic images, the canal ramifications or divisions were also evident and recorded.
The single root canal divisions or ramifications in our study were noted most commonly in the middle and apical 1/3rd levels of the teeth and most commonly found in Type V. These results were comparable and in agreement with studies in mandibular premolars from the western Chinese population and Shanghai (87% and 75% in first and second premolars) [20-22]; India [23]; Venezuela [24]; Spain [25] and Iran [26]. There is a higher prevalence of multiple root canals with complex morphologies which can be best visualized with 3D imaging [20, 21, 23-29]. The two most prevalent canal types of root canals reported in the literature are Type I and Type V [12, 13, 20, 21, 23, 28, 29].
The present study results were in contradiction to another similar study conducted on mandibular first premolars in Saudi Arabia on 216 teeth. Type I was the most prevalent root canal morphological type, especially in single-rooted teeth (74%), and Type V was the most common type in two-rooted mandibular first premolar (55.5%) [30]. In this study, the male gender had more occurrence of two canals, which is in alignment with the observation in our present study. Another study in different geographical locations in the same country revealed 99.1% of canals as Type I [30, 31]. The results of the study highlight the possibility of variations in root canal morphology other than Vertucci’s classification which is coherent as in multiple studies using micro-computed tomography for root canal morphology [32-35].
There exist no clear criteria to differentiate the ramifications of the root canal from lateral or secondary canals [36]. With an increase in research with various imaging methods, many of the formerly unreported anatomical complexities are brought to attention [32, 37-39]. The new root canal classification system is an eye opener to the changes in root canal classification in which every possible detail in classifying root canals and canal morphology was done [36].
The fact that despite the advent of three-dimensional imaging, the majority of the research published using CBCT follows the conventional root canal classification by Vertucci many decades ago which gives a two-dimensional classification approach. The researchers of the majority of these publications do not have an oral radiologist involved in the research and are not experts or students who were not calibrated with no interexaminer reliability agreement carried out before the investigations [29, 40-45]. This explains the reason why the current research is still held with Vertucci's classification of type I as the most common root configuration type. This aspect has to be further explored.
Also, several micro-CT studies have shown variations in root canal morphologies apart from the conventional classification of type I canal as well as found that the majority of teeth examined have more than 1 canal [7, 46, 47].
The current study was conducted with adequate samples to be considered generalizable. Future multicenter studies should be conducted in the same population with a different 3d imaging source of cone beam computed tomography with experienced and calibrated investigators, in a large sample size from the same ethnic sample. The researchers should explore the possibilities of 3d imaging to find a difference from the conventional methods of classification.
Conclusion
The most common root canal configurations found in the study were Type V and Type I. Mandibular premolars depicted complex root canal morphologies and can be associated with the presence of radicular grooves. The study also highlights the need to revisit the classification of root canals based on advanced cone beam computed tomography that gives more details than the conventional 2 D radiograph-based classifications.
From a clinician’s perspective, such anatomical variations of the mandibular premolar require the endodontists to be alert to prevent root canal failures. The knowledge and understanding of such complex morphological root canal variations can contribute to the achievement of more success in endodontic therapy.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: The study was approved by the institutional review board (RC/IRB/2019/308).