Several factors affect the quality of Complete denture (CD) final impressions, such as techniques, materials, operator skills, and dentist-patient relationship. Hence, understanding the clinical impressions-related skills of students may help improve the assessment and teaching process. A total of 160 completely edentulous arches were treated, maxillary (n=80) and mandibular (n=80). Final impressions were made by 4th-year undergraduate dental students (males=40 and females=40). The defects and quality of the impressions were assessed and evaluated using a calibrated grading model. Using the grading model for evaluating impressions showed that the mean quality grades of maxillary and mandibular arch impressions were 8.62 ± 1.7 and 7.29 ± 2.1 (12 the highest), suggesting that students made higher quality impressions on average. There was a significant difference (p < 0.001) between the mean quality grade of impressions made by the students, implying that maxillary impressions made by females were significantly of higher quality than males. There were significant differences (p = 0.003) between the overall qualities of both arch impressions, suggesting that maxillary impressions were significantly made of higher quality compared to mandibular impressions regardless of the gender of students. Overall, undergraduate dental students made better-quality impressions. Female students constructed impressions of higher quality than males, and maxillary impressions were made with better quality compared to mandibular impressions. The calibrated grading method developed for this research may uniform the evaluation of the impressions and improve clinical teaching, thereby developing competent dentists who provide good patient care and satisfaction.
Introduction
The treatment of edentulous patients having complete dentures (CD) prostheses is considered a technically demanding procedure for dentists [1]. The accuracy in recording the CD foundation intraorally depends on several factors, such as the understanding of the impression technique and material used, the operator skill, and the dentist-patient relationship [2, 3]. In undergraduate dental teaching, students are taught to acquire clinical skills in CD construction. The definitive (final, secondary, and working) impression stage in the CD construction procedure is a critical step for the success of the final prosthesis for obtaining an accurate impression of the denture-associated areas in the edentulous jaws, considering minimal distortion of the alveolar ridge and border tissues [4-6]. An accurate definitive impression considers a retentive prosthesis with optimum aesthetics, and function and with a comfortable fit for edentulous patients [5]. Therefore, a well-constructed CD will minimize the amount of CD irritation and the need for adjustment or remaking [1]. The understanding of facial and intraoral muscle function and intraoral and extraoral landmarks are all necessary to record all the required landmarks a master (working) cast that replicate the residual ridge of the patient and the reflection of the surrounding soft tissues [1, 2].
A minimally acceptable protocol (MAP) was proposed to assess the clinical techniques of CD construction, including impression-making [7]. For problems associated with CD during function, aesthetics could be traced back to the origin of the defect during CD construction, one of which is the impression-making stage [8, 9]. Consequently, final impression-making may be a challenging skill in the CD construction procedure to be mastered by undergraduate dental students who have limited clinical experience [6]. Rodegerdts used a grading method for detecting pressure areas in complete dentures [10]. The use of this method may allow the understanding of the clinical impression skills of students in terms of evaluating the quality and defects made by the students. Hence, this may help in improving the teaching process in CD clinical training to develop competent dentists.
This study aimed to determine the quality and defects present in final impressions for both maxillary and mandibular arches made by 4th-year dental students by using the same impression technique.
Materials and Methods
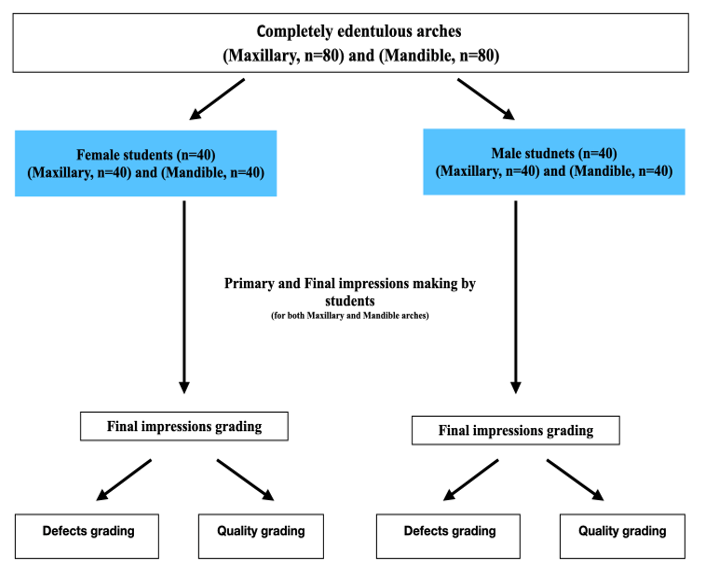
The approval to conduct this study was obtained from the ethical committee of the faculty of dentistry. Eighty (n=80) completely edentulous patients, having edentulous maxillary and mandible arches, were selected from the outpatient clinic, removable prosthodontics division, faculty of dentistry, King Abdulaziz University Dental Hospital. After securing consent, the patients were selected to be treated in the completed denture course given to 4th-year undergraduate dental students. For the level of the students and standardization of the study, the following criteria were used: no previous CD experience, healthy oral mucosa, and typically formed residual ridges with the least possible undercuts. Eighty equally male (n=40) and female (n=40) 4th-year undergraduate dental student representatives were tasked to construct the necessary impressions for the patients. They practiced making impressions twice, having the third attempt-made impressions collected and used for the actual analysis. The study design of the research includes the following steps: a) primary impressions, b) final impressions, and c) impression defects and quality grading (Figure 1).
|
|
|
Figure 1. Flow chart of the study design |
Primary impressions
These were made by each student using perforated metal stock trays, utility wax, and alginate impression material of regular set (Feltrate, Desply, Ltd, UK). After disinfection of the impressions, pouring was performed immediately. Each cast was outlined correctly, and a layer of base plate wax was applied as a spacer. Custom impression trays with 4 stoppers and L-shaped handles were constructed using VLC resin (Techno Tray L U Z, Protectino, Spain). Trays were checked intra-orally to ensure that the tray borders were about 2-3 mm shorter than the relaxing vestibuler reflections. Tray border molding was done entirely by each student using an open-mouth technique through the use of a low-fusing compound (KEMCO, Green Tracing Sticks, Kemdent Work, UK). After the removal of excess material and scraping of border material, trays were painted with tray adhesive (Universal Tray Adhesive, Thermak, SPA, Italy) and allowed to air dry. A monophase polyvinyl silicosan impression material of a regular set (Variotime, Kulzer Gmbh, Germany) was used for making the final impression. The final impression material was loaded in each custom tray using an automix gun with a standard syringe tip diameter. The impression material was evenly distributed in the trays using an aseptic tongue depressor. The final impressions were made using the open-mouth technique. After impression making, each maxillary and mandibular impression was disinfected, collected, and given a code number after each clinical session. Also, each maxillary and mandibular final impression was assessed by visual inspection after calibration by three investigators.
Final impression
The final impressions were made in a border-molded custom tray technique [11] for the fabrication of a conventional CD for completely edentulous patients.
Evaluation and grading of final impressions
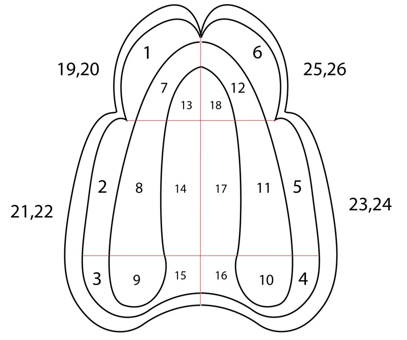
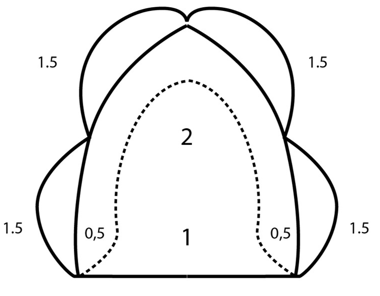
The evaluation was done using a grading model. This model divided the surfaces of the impressions into 26 zones for the maxillary arch and 24 zones for the mandible arch (Figures 2 and 3). The defects and quality of final impressions were evaluated according to calibrated grading diagrammatic charts developed by the authors. The defects of the impressions were defined according to their location (zones) in the arch impression. In addition, the quality of the impressions was defined according to their location (zones) in the arch impression and graded out of 10 in both arches. The authors subjectively graded the overall surfaces and extensions (Figures 2 and 3).
Statistical analysis
Data collected were analyzed using GraphPad Prism version 8 (GraphPad Software, Inc., San Diego, CA, USA). Simple descriptive statistics were used to characterize the study variables. The categorical and numerical variables were presented in the form of counts and percentages, while continuous variables were reported as means and standard deviations. The chi-square and Fisher’s Exact tests were used to show the relationship between categorical variables, while the Mann-Whitney test was used for comparing two group means. Moreover, a Paired-Samples T-test was used to compare the means of two variables for a single group, to compute the differences between values of the two variables for each case, and to test whether the average differs from 0. Lastly, a conventional p-value of 0.05 was the criteria to reject the null hypothesis.
|
|
|
a) |
|
|
|
b) |
|
Figure 3. Mandibular arch impression recording charts. a) Zone-assigned diagram: The surface of the impression was divided into 12 zones to locate the errors in students-made impressions. Zone assignments were 1-4 zones for labial and buccal surfaces of the alveolar ridge, 5 and 6 zones for the lingual surface, and 7 to 12 zones for the alveolar ridge. Extensions for borders were given numbers 13, 15, 17, 19, 21, and 23. Numbers 14, 16, 18, 20, 22, and 24 were assigned for border thickness. b) Quality-graded diagram: The surface includes a total of 10 grades for the assessment of the students-made impression quality. In addition, two grades were added for the assessment of the thickness. |
Results and Discussion
The defects present in the final impressions of both arches were divided into common and less common defects according to their frequency. The maxillary impression defects assessment results shown in (Table 1) represent the proportions of defects in all areas of final impressions made by both males and females for maxillary arch impressions. Overall, no significant differences (p > 0.05) were found among the most common defects, such as pressure area, border extensions (over and under), and border thickness (thin versus thick).
Table 1. Summary proportions of defects in all areas of male (M) and female (F) made maxillary arch impressions.
|
Variables |
Most common |
Control |
Least common |
|||||
|
M |
F |
p-value |
M |
F |
p-value |
M |
F |
|
|
Pressure areas |
10 |
11 |
0.799 |
4 |
4 |
1.000 |
2 |
2 |
|
Voids area |
NA |
NA |
- |
26 |
34 |
0.039* |
2 |
1 |
|
Border extension (Over) |
25 |
20 |
0.260 |
8 |
5 |
0.363 |
0 |
2 |
|
Border extension (Under) |
9 |
5 |
0.239 |
24 |
26 |
0.644 |
0 |
2 |
|
p-value |
0.564a |
|
|
|
|
|
|
|
|
Border thickness (Thin) |
9 |
4 |
0.130 |
26 |
28 |
0.633 |
2 |
3 |
|
Border thickness (Thick) |
25 |
19 |
0.178 |
4 |
5 |
1.000 |
0 |
1 |
|
p-value |
0.423b |
|
|
|
|
|
||
|
*-Significant using Chi-Square Test @<0.05 level. a-comparison between Border extension Over vs. Under b-comparison between Border thickness Thin vs. Thin |
||||||||
However, for the mandibular arch final impressions, there were significant differences among the most common defects in terms of border extension (over) (p = 0.039) with respect to both genders according to the Chi-square test (Table 2). This suggests that a significantly higher number of male students committed the most common defect in this area compared to females. While the rest of the defects showed no significant differences (p > 0.05). Also, there were no significant differences between the most common defects in terms of comparison of border extensions (over versus under; p > 0.05) and border thickness (thin versus thick; p > 0.05) relative to both genders.
Table 2. Summary proportions of defects in all areas of male- and female-made mandibular arch impressions.
|
Variables |
Most common |
Control |
Least common |
|||||
|
Male |
Female |
p-value |
Male |
Female |
p-value |
Male |
Female |
|
|
Pressure areas |
12 |
12 |
1.000 |
4 |
1 |
0.359 |
2 |
3 |
|
Voids area |
1 |
1 |
1.000 |
38 |
39 |
1.000 |
NA |
NA |
|
Border extension (Over) |
29 |
20 |
0.039* |
2 |
4 |
0.675 |
1 |
1 |
|
Border extension (Under) |
7 |
6 |
0.762 |
22 |
22 |
1.000 |
1 |
2 |
|
p-value |
0.729a |
|
|
|
|
|
|
|
|
Border thickness (Thin) |
7 |
5 |
0.531 |
22 |
28 |
0.166 |
2 |
2 |
|
Border thickness (Thick) |
20 |
15 |
0.223 |
6 |
7 |
0.762 |
0 |
1 |
|
p-value |
0.943b |
|
|
|
|
|
||
|
*-Significant using Chi-Square Test @<0.05 level. |
||||||||
There were no significant differences observed for both the most and least common defects in both maxillary and mandibular arch impressions in terms of all variables (p > 0.05), with respect to both male and female genders (Table 3). Additionally, there were no significant differences between the most common defects in both maxillary and mandibular arch impressions in terms of comparison of border extensions (over versus under; p > 0.05) and border thickness (thin versus thick; p > 0.05) regardless of gender of students.
Table 3. Overall summary proportions of defects in all areas of male- and female-made maxillary (Max) and mandible (Mand) arch impressions.
|
Variables |
Most common |
Control |
Least common |
|||||||
|
Max |
Mand |
Aver-age |
p-value |
Max |
Mand |
Aver-age |
p-value |
Max |
Mand |
|
|
Pressure areas |
10 |
12 |
11 |
0.617 |
4 |
3 |
4 |
0.692 |
2 |
3 |
|
Voids area |
NA |
1 |
- |
- |
30 |
39 |
35 |
0.004* |
2 |
NA |
|
Border extension (Over) |
23 |
25 |
24 |
0.648 |
7 |
3 |
5 |
0.176 |
1 |
1 |
|
Border extension (Under) |
7 |
7 |
7 |
1.000 |
25 |
22 |
24 |
0.496 |
1 |
2 |
|
p-value |
0.891a |
|
|
|
|
|
|
|
|
|
|
Border thickness (Thin) |
7 |
6 |
7 |
0.762 |
27 |
25 |
26 |
0.639 |
3 |
2 |
|
Border thickness (Thick) |
22 |
18 |
20 |
0.371 |
5 |
7 |
6 |
0.531 |
1 |
1 |
|
p-value |
0.942b |
|
|
|
|
|
|
|
|
|
|
*-Significant using Chi-Square Test @<0.05 level. a-comparison between Border extension Over vs. Under b-comparison between Border thickness Thin vs. Thin |
||||||||||
When comparing the overall quality of both maxillary and mandibular arch impressions, the result revealed that there were significant differences (p =0 .003) between the two, resulting in 1.330 mean differences, according to the Paired Sample t-test (Table 4). This implies that maxillary arch impressions were significantly made of higher quality compared to mandibular arch impressions regardless of the gender of students.
Table 4. The overall average quality of male- and female-made maxillary and mandibular arch impressions.
|
Quality |
Maxillary |
Mandibular |
Average Total |
Mean Difference |
95% C.I. |
p-value |
|
Mean ± SD |
8.62 ± 1.7 |
7.29 ± 2.1 |
7.96 ± 1.9 |
1.330 |
0.480-2.181 |
0.003* |
|
Median |
8.9 |
7.5 |
8.2 |
|||
|
*-significant using Paired Sample t-test @<0.05 level |
||||||
In this study, the same impression technique and materials were used to lessen the distortion of ridge and border tissues, thereby minimizing the effect of these variables and mainly focusing on gender factors. In addition, there is no available evidence that supports one technique or material over another for making CD prostheses [5]. PVS was used due to its favorable qualities, relative simplicity and reliability, and its wide use by dental practitioners [5, 11-13]. In terms of defect assessment, more than 50% of students in the present study constructed defects related to pressure area, border extension (over), and border thickness (thick) for both maxillary and mandibular arch impressions. This was also observed in the study of Woelfel and colleagues (1963), wherein the greatest variations in the border contour (around the buccal frenum region), the thickness of the impression material (over the posterior post palatal area), and difference in the pressure areas (size and location) were found on an edentulous ridge-impressions constructed by seven dentists for the same patient despite their more clinical experience [14]. On the other hand, most of the students in the present study did not produce voids. The syringe tip diameter used was the same for each impression material. Impression material tip diameter has been identified as a causative factor that may influence the number of voids present in the syringe [15]. Furthermore, a tongue depressor was used to spread the impression in an even manner throughout the tray, thereby producing a smooth surface free from voids [16]. No significant defects were observed for the post-palatal area in maxillary arch impressions. This can be attributed to the customized trays, which were made with visible light-cured tray material (with adequate spacer) by technicians [1, 3, 5].
Overall, female students made better quality impressions compared to male students. In a retrospective study by Sawair and co-workers (2009) in Jordan, female dental students were also found to perform better in prosthodontics (theoretical and clinical) in general compared to males [17, 18]. Several studies showed that several factors influenced the performance of academic students, such as young age, part-time work, smoking habits, and sleep problems [19]. Though 4th-year female students made better-quality impressions over the males, results of the present study showed that both genders made quality arch impressions (maxillary and mandibular) on average. This suggests that the students had enough confidence in constructing impressions and had proper clinical training, specifically understanding mistakes and considering critical feedback from clinical supervisors [17]. In an anonymous cross-sectional survey of dental undergraduates (Years 3 – 5) in Portugal, results revealed that the perception of confidence of students, along with treating partial and complete dentures, became higher as the year of studies progressed. These students mentioned that they were satisfied with their prosthodontic learning, especially in clinical training [20]. The national survey conducted on young dentists in Finland by Karaharju-Suvanto and colleagues (2014) also revealed that students were relatively well-equipped to work as dentists and that dental education for undergraduates has satisfied the necessary skills for clinical practice [21]. Moreover, the positive role of clinical supervisors in terms of critical and constructive feedback may encourage deep learning and excellent clinical skills [22].
The description of the “quality” of arch impressions in this study was only limited to the personal evaluation of the dental students based on a standard method [1, 7]. Conducting additional studies on the confidence of the students in creating impressions and impression-user satisfaction may also further expand the definition of “quality” for both male- and female students-made impressions. The relationship between the perception of dental students on the quality of teaching and the quality of their constructed impressions can also be investigated. Improving dental education may continually help in producing more competent future dentists and minimize the learning differences between genders, especially in prosthodontics.
The numerical grading model developed was used in this study to assist clinical supervisors in evaluating students’ impression-making as well as providing students with a teaching tool. Allowing undergraduate students to learn from their defects and the quality of their impression-making by practice and having feedback from their supervisors in their early clinical experience is essential to enhancing their confidence and skills [10, 23]. Therefore, the proposed model could offer valuable training experience for undergraduate students to become competent general dentists.
Conclusion
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: The study fulfills the ethical requirements of King Abdulaziz University.