To prepare and characterize linezolid-based hydrogel and evaluate its efficacy as local drug delivery in stage II grade A periodontitis. Linezolid-based hydrogel was prepared. Hemolysis assay was done at various concentrations (2%, 4%, 6%, 8%, 10%) and a biocompatibility test was performed by MTT Assay. Forty patients with stage II grade A periodontitis were involved in this clinical trial. Participants were split into two groups. Group A (control) received only scaling and root planing (SRP) and Group B (test) received linezolid gel along with SRP. Clinical data were recorded, including plaque index (PI), gingival index (GI), probing pocket depth (PPD), clinical attachment level (CAL) at baseline and after 3 months. In vitro analysis revealed that at 2% concentration, the hemolysis ratio was less than 1% and 98% cell viability was observed after 94 hours in biocompatibility assay. 2% Linezolid-based hydrogel was subjected to in vivo analysis. Upon intra-group comparison, all the clinical parameters (PI, GI, PPD, CAL) showed statistically significant differences (p<0.05) from baseline to 3 months. Also on the inter-group comparison, a significant difference was evident in all parameters in favor of Group B (p<0.05). For patients with stage II grade A periodontitis, locally administered linezolid gel seems to be effective as an adjunct to SRP.
Introduction
Periodontitis is a chronic inflammatory multifactorial disease that destroys tooth-supporting structures. Although various etiologies contribute to the course of disease, the presence of bacteria plays an important role in disease initiation. Periodontitis begins and progresses due to dysbiosis of the microbiota and disturbed host defenses [1]. Oral commensals in healthy periodontium include Streptococci, Capnocytophaga, Corynebacterium, Actinomyces, and Veillonella genera [2, 3]. Oral commensals lay the foundation for subgingival pathobiont growth, which results in dysbiosis of the microbiota. Commensals interact with late-arriving pathobionts in a variety of ways that influence the expression of their virulence factors, colonization, and accumulation during the microbiota's transition from a healthy to a pathogenic state [4]. In a diseased state, Porphyromonas gingivalis, Treponema denticola, Tannerella forsythia, and Fusobacterium nucleatum are significant pathobionts that are closely related to subgingival plaque [5]. The majority of the pathogenicity of pathobionts is attributed to their metabolic activities, which are also crucial in host-microbe interactions. These microbial metabolites are harmful to host cells and tissues [6].
Periodontitis is often treated with mechanical debridement of the affected root surface in an effort to reduce the bacterial load and alter the environmental parameters of these microbial habitats. Winkel et al. proposed that antimicrobial therapy as an adjunct to mechanical debridement would improve the clinical outcome, and would even be essential for a successful treatment [7]. Thereafter, the treatment of periodontitis has involved the local administration of many antibiotics [8-10].
Linezolid belongs to a novel class of antibiotics called oxazolidinones, which treats infections caused by aerobes and anaerobes that are sensitive to other group of drugs [11]. Linezolid interacts with the 50S ribosomal subunit to prevent the synthesis of proteins. It has great oral absorption, good pharmacokinetic/ pharmacodynamic characteristics, and inhibits biofilm formation [12].
Researchers have reported that systemic drug delivery in addition to mechanical debridement resulted in an increased rate of tolerance. Frequent administration of large dosages or repeated administration in order to provide a therapeutic effect resulted in harmful side effects, including systemic toxicity [13, 14]. Controlled local delivery of the anti-bacterial and anti-inflammatory drugs was subsequently developed and is found to be more effective at maintaining the drug concentration in the periodontal pocket than the systemic approach [15]. Furthermore, controlled local drug delivery includes various methods such as oral irrigation, fibers, vesicles, strips, gels, and microparticulate systems [16-18]. Among these, the hydrogel delivery approach can regulate the release of various therapeutic substances, including small-molecule medicines, macromolecular medications, and cells [19, 20]. These hydrogels have the capacity to control the quantity of drugs that are delivered to reach cells and tissues over time and in different sites [21].
In literature, various hydrogels have been used as an adjunct to SRP. Experimental studies have proved that hydrogels have the property of controlled release of drug [22] and facilitate periodontal wound healing [23]. Furthermore, it has been reported that hydrogels are an effective mode of local drug delivery in the management of periodontitis [24]. In this context, the goal of this study was to formulate linezolid-based hydrogel and evaluate its efficacy as a locally delivered drug in the management of stage II grade A periodontitis.
Materials and Methods
Linezolid hydrogel preparation
Sodium alginate solution (2%, w/v) and hyaluronic acid solution (2%, w/v) were prepared by adding 2 gm sodium alginate and 2 gm hyaluronic acid in 100 ml deionized water at room temperature separately. A hydrogel solution was prepared adding both sodium alginate solution and hyaluronic acid solution at 2:1 ratio respectively. Using a magnetic stirrer, a uniform mixture was obtained after 2 hours of stirring. Then 0.2% w/v of linezolid was added into that mixture and kept in the stirrer for another 30 mins. Further linezolid hydrogel was ion-cross linked in 200 mM calcium chloride for 24 hours. Then, the linezolid hydrogel was taken to further experiments.
In vitro analysis
Hemolysis assay
4 ml of fresh anticoagulant (EDTA) whole blood was diluted with 5 milliliters of 0.9 weight percent NaCl solution to create the diluted whole blood solution. The 50μL sample was added into 950μL of 1x PBS solution in a 1.5ml Eppendorf centrifuge tube and incubated at 37 °C for 30 mins. Further 0.2 mL diluted whole blood was added and incubated at 37 °C for 1 h. The solution was centrifuged at 1000 rpm for 10 mins, and after that, a UV spectrophotometer was used to test the supernatant's absorbance at 545 nm.
Biocompatibility assay
The biocompatibility of linezolid hydrogel along with control (placebo gel) treated on human periodontal ligament tissue-derived primary cells (fibroblasts) was determined over 24 hours by MTT assay. Linezolid hydrogel in different percentages incubated on fibroblast cells was seeded in 96 well culture plates for 24 hours. To determine percent cell viability, the post-incubated cells were replaced with 10 𝜇l of stock MTT dye (10 mg/ml), which was added to each well culture plate and incubated at 37 °C for 4 hours. To dissolve the formazan crystals, the medium was replaced with 100 μl dimethyl sulfoxide in each well, and absorbance was recorded at 570 nm with the Synergy Hybrid Multi-Mode Reader (BioTek, Winooski, VT, US).
In vivo analysis
Patient selection
Forty outpatients from the Department of Periodontology, Saveetha Dental College and Hospitals, Chennai were selected for this study. Patients of both genders of age between 25 to 55 years diagnosed with stage II grade A periodontitis and the presence of at least 20 natural teeth were considered for this study. Patients under antimicrobial or antibiotic drugs for the past 3 months, systemically compromised, pregnant women, lactating mothers, and smokers were excluded from this study.
Study protocol
The study protocol was approved by the Institutional Review and Ethical Committee of Saveetha Dental College and Hospitals, Chennai, India prior to commencing this investigation (Reference number: IHEC/SDC/PERIO-2204/23/327). Also, every individual involved in the research gave their informed consent. G Power software, Version 3.1.9.4 was used to determine the sample size which came out to be 40 (power at 80% and alpha error at 95% confidence level) by considering the mean and standard deviation values from the earlier research [25].
This clinical study was performed to evaluate the efficacy of linezolid hydrogel as local drug delivery as an adjunct to scaling and root planing (SRP) in the management of stage II grade A periodontitis. 20 patients were subjected to SRP alone (Group A - Control) and the remaining 20 patients were subjected to SRP + linezolid hydrogel (Group B - Test).
Clinical parameters
The clinical parameters recorded were 1. Plaque Index (PI) (Silness and Loe, 1964) 2. Gingival Index (GI) (Loe and Silness, 1963) 3. Probing Pocket Depth (PPD) 4. Clinical Attachment Level (CAL). All these information were recorded at baseline and 3 months.
Periodontal therapy
All patients in this study were treated with scaling and root planing using an ultrasonic scaler and hand instruments (Gracey curettes, Hu-Friedy®, Chicago, IL, USA). Group B patients were treated with scaling and root planing and linezolid hydrogel. Hydrogel was injected subgingivally into the periodontal pocket using a blunt cannula syringe. In both groups, periodontal dressing was placed. For one week, the participants were instructed not to use any interdental appliances, chew hard meals, or consume sticky foods. They were also told not to brush in the vicinity of the treated areas. After 1-week, periodontal dressing was removed. Patients were recalled for review after 3 months.
Statistical analysis
Using SPSS software, Version 23.0, statistical analysis was carried out. The normality distribution of data was done using the Shapiro-Wilk test. An independent t-test was used to evaluate the intergroup comparison. Within-group comparison between baseline and 3 months was analyzed by paired t-test. P value less than 0.05 was considered as a statistically significant difference.
Results and Discussion
In vitro analysis
Hemolysis assay
The hemolysis ratio has been recorded at different concentrations of hydrogel. At 2% concentration, the hemolysis ratio was less than 1%, and at 4%, 6%, 8%,10% concentrations, the hemolysis ratio was less than 2%. This finding indicated that the linezolid hydrogels had a low red blood cell destruction ratio (Figure 1).
|
|
|
Figure 1. Hemolysis assay |
Biocompatibility assay
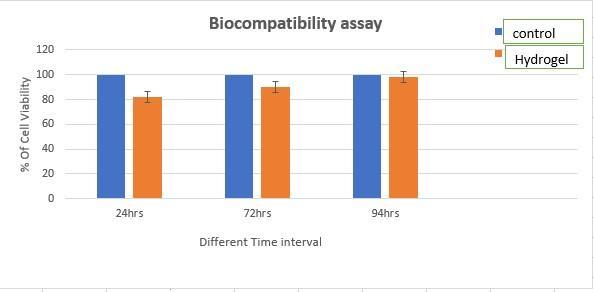
Human periodontal ligament tissue-derived fibroblasts were treated with different concentrations of linezolid hydrogel for 24 hours, 72 hours, and 94 hours. Then, an MTT assay was used to evaluate the cell viability and data were normalized to unexposed cells. It was seen that after 24 hours, cell viability reduced up to 80% in the hydrogel, at 72 hours cell viability was 90% and after 94 hours cell viability was 98% which represents that after 94 hours, linezolid hydrogel does not exhibit a significant toxic effect on human fibroblasts (Figure 2).
|
|
|
Figure 2. Biocompatibility assay |
In vivo analysis
Table 1 summarizes the clinical and demographic features of both groups. Patients treated with only scaling and root planing (Group A) presented with a mean of age 42.40 ± 3.27 years, PI of 2.63±0.19 mm, GI of 2.60±0.22 mm, PPD of 5.69±0.36 mm, CAL of 5.91±0.38 mm. There were 9 male and 11 female participants. Patients treated with SRP along with Hydrogel (Group B) presented with a mean age of 41.59 ± 3.35 years, PI of 2.67±0.20 mm, GI of 2.63±0.20 mm, PPD of 5.73±0.39 mm, CAL of 5.92±0.41 mm. There were 11 male and 9 female participants.
Table 2 depicts the comparison between two groups SRP (Group A) and SRP with Hydrogel (Group B) at baseline and after 3 months using independent t-tests. Baseline mean values of all parameters PI, GI, PPD, and CAL of both the groups have no marked difference (p>0.05). Whereas, there was a statistically significant difference observed after three months in all parameters PI, GI, PPD, and CAL in favor of Group B (SRP + Gel) when compared to Group A (SRP alone) with a p-value of 0.00.
Table 3 depicts a comparison between baseline and after 3 months in both groups using paired t-tests. In Group A, PI value was reduced from 2.63±0.19 mm to 1.29±0.29 mm, GI was reduced from 2.60±0.22 mm to 1.58±0.31mm, PPD was reduced from 5.69±0.36 mm to 3.96±0.70 mm, CAL was reduced from 5.91±0.38 mm to 4.18±0.68 mm. There were significant differences observed in all parameters PI, GI, PPD, and CAL with p-value <0.05. Whereas in Group B (SRP + Gel) PI value was reduced from 2.67±0.20 mm to 0.48±0.20 mm, GI was reduced from 2.63±0.20 mm to 0.72±0.21mm, PPD was reduced from 5.73±0.39 mm to 3.08±0.34 mm, CAL was reduced from 5.92±0.41 mm to 3.27±0.35 mm. There were significant differences observed in all parameters PI, GI, PPD, and CAL with p-value <0.05. There was a greater improvement in Group B as compared to Group A in all parameters at 3rd month follow-up.
Table 1. Demographic and clinical characteristics of the study population of both groups
|
Parameter |
Group A |
Group B |
p-value |
|
Age |
42.40 ± 3.27 |
41.59 ± 3.35 |
0.62 |
|
Gender (Male/ Female) |
9/11 |
11/9 |
0.41 |
|
PI |
2.63±0.19 |
2.67±0.20 |
0.53 |
|
GI |
2.60±0.22 |
2.63±0.20 |
0.60 |
|
PPD |
5.69±0.36 |
5.73±0.39 |
0.74 |
|
CAL |
5.91±0.38 |
5.92±0.41 |
0.96 |
Table 2. Comparison of clinical parameters between two groups by independent t-test
|
Parameters |
Timeline |
Group A (Mean±SD) |
Group B (Mean±SD) |
p-value |
|
PI |
Baseline |
2.63±0.19 |
2.67±0.20 |
0.53 |
|
3 month |
1.29±0.29 |
0.48±0.20 |
0.00* |
|
|
GI |
Baseline |
2.60±0.22 |
2.63±0.20 |
0.60 |
|
3 month |
1.58±0.31 |
0.72±0.21 |
0.00* |
|
|
PPD |
Baseline |
5.69±0.36 |
5.73±0.39 |
0.74 |
|
3 month |
3.96±0.70 |
3.08±0.34 |
0.00* |
|
|
CAL |
Baseline |
5.91±0.38 |
5.92±0.41 |
0.96 |
|
3 month |
4.18±0.68 |
3.27±0.35 |
0.00* |
*Statistically significant at p-value <0.05
Table 3. Comparison of mean clinical parameters between baseline and 3 months in group A and group B by paired t-test
|
Parameters |
Timeline |
Group A (Mean±SD) |
p-value |
Group B (Mean±SD) |
p-value |
|
PI |
Baseline |
2.63±0.19 |
0.00* |
2.67±0.20 |
0.00* |
|
3 month |
1.29±0.29 |
0.48±0.20 |
|||
|
GI |
Baseline |
2.60±0.22 |
0.00* |
2.63±0.20 |
0.00* |
|
3 month |
1.58±0.31 |
0.72±0.21 |
|||
|
PPD |
Baseline |
5.69±0.36 |
0.00* |
5.73±0.39 |
0.00* |
|
3 month |
3.96±0.70 |
3.08±0.34 |
|||
|
CAL |
Baseline |
5.91±0.38 |
0.00* |
5.92±0.41 |
0.00* |
|
3 month |
4.18±0.68 |
3.27±0.35 |
*Statistically significant at p-value <0.05
In recent days, local drug delivery for the management of periodontal disease has drawn a lot of attention and investigation. This method enables the targeted and regulated release of medications by administering therapeutic chemicals directly to the site of infection or inflammation. Literature evidence has shown linezolid targets aerobes, anaerobes and inhibits biofilm formation [12]. Also, literature shows that hydrogels can provide sustained release of drugs over an extended period. It can adhere to periodontal tissue allowing targeted drug delivery in affected areas [19]. This study aimed to formulate linezolid-based hydrogel and evaluate its efficacy as a locally delivered drug in the management of stage II grade A periodontitis.
An ideal local drug delivery agent should possess various characteristics which include good biocompatibility, and good hemostatic ability [26]. In the present study, linezolid hydrogel was prepared, and then a hemolytic analysis and biocompatibility test were performed. It has been observed that linezolid hydrogel has a low red blood cell destruction ratio and it is considered a non-significant toxic substance. The characterization analysis proved that the developed hydrogel is an ideal local drug delivery agent.
Goudanavar et al. prepared and characterized linezolid in-situ gel for the treatment of periodontitis. pH-sensitive in-situ gel was prepared using carbopol 934P and hydroxypropyl methylcellulose and carbopol 934P and sodium carboxymethylcellulose utilizing the cold method. The in-situ gels that were prepared underwent assessments for their appearance, pH, gelling capability, viscosity, rheological investigations, in vitro release tests, and drug content estimation before being put through an antibacterial activity test. Results revealed that the drug and physical mixture were compatible with each other. The prepared formulation showed drug release up to 12 hrs [27]. Furthermore, Wassif et al. developed hydrogel filled with spray-dried polymeric nanoparticles containing both linezolid and nanohydroxyapatite and tested in animal models with bone infections. The authors reported that within 2-4 weeks of injection, they succeeded in controlling the bone infections [28].
As it was proven that linezolid was effective in bone infections, in the present study the prepared linezolid hydrogel was subjected to a clinical trial among stage II grade A periodontitis patients. There was a significant reduction in clinical parameters like PI, GI, PPD, and CAL among patients treated with SRP and hydrogel when compared to patients with SRP alone. The current research's results cannot be directly compared to those of any other study since it is the first study of its type to assess the efficacy of linezolid hydrogel as a local drug delivery agent in the management of periodontitis. However, the results in the current research are indirectly in line with previous studies, where other antibiotics have been used as an adjunct to SRP as local drug delivery in periodontitis patients.
Graca et al. employed 2% minocycline as a local drug delivery method for patients with periodontitis and noted a significant decrease in PD from baseline to 6 and 12 weeks [29]. Sharma et al. reported that usage of 1% alendronate gel as a local drug delivery system resulted in a marked reduction in PD and CAL at 2nd and 6th months [30]. Also, when 3% satranidazole gel was used as an adjunct to SRP, improvements in periodontal parameters were reported [31]. Our findings are following the previous studies.
Overall, the developed linezolid hydrogel is proven to be biocompatible and has hemostatic properties. Also, the clinical study suggests that linezolid hydrogel is effective when used in addition to scaling and root planing as a local drug delivery among stage II grade A periodontitis patients.
However, this study has few limitations. The in vitro study fails to analyze the release pattern and also degradation rate. Also, the clinical study was done among a small number of patients. Therefore, further randomized controlled trials are needed to be conducted among larger groups of the population to substantiate the study findings.
Conclusion
The study findings suggest that for patients with stage II grade A periodontitis, locally administered linezolid gel as an adjunct to SRP seems to be effective in significant improvement in clinical parameters including plaque index, gingival index, probing pocket depth and clinical attachment level.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None