Although molar distalization is one of the most difficult movements to achieve with conventional orthodontic treatment, it has been reported that it is one of the most predictable movement when using clear aligners. The aim of this systematic review is to assess the efficiency of molar distalization using clear aligners, and to evaluate the associated effects of this treatment. Pubmed, Scoups, science direct, Web of Science, and EBSCO databases were searched up to May 2023 for randomized controlled trials (RCTs) and non-randomized prospective and retrospective studies on maxillary and lower molar distalization using clear aligner. Ten studies were included in the systematic review, two prospective non-randomized and eight retrospective non-randomized. The predictability of molar distalization ranges from 31.1% to 87%, with good control of the vertical dimension and tipping movements. The lower molar distalization is mainly a tipping movement rather than bodily movement. Molar distalization using clear aligners appears to be effective, although variations in study protocols may contribute to differences in predictability rates. Randomized controlled trials with standardized protocols are therefore needed to provide more accurate assessments.
Introduction
Molar distalization is the term used to describe the rearward migration of teeth that corrects the connection between molars and lengthens the dental arch to acquire space. Its main indication is sagittal arch length discrepancy when extraction is not desirable [1, 2]. Multiple treatment methods and appliances have been described for molar distalization, can be extra-orally or intra-orally [3, 4]. This distalization movement may have undesired side effects such as molar extrusion and tipping; loss of anchorage of anterior teeth, which manifests as fared incisors and the protrusion of lips [5, 6]. which require good anchorage control.
Over the past twenty years, the use of removable transparent aligners for orthodontic treatment has increased in popularity. This is largely because more and more patients are seeking more comfortable and aesthetically pleasing options than traditional fixed orthodontic appliances. As a result, clear aligner (CA) technology has been developed and matured [7, 8].
Clear aligners are quite successful in treating a variety of malocclusions, including severe crowding, open bite, cross bite, deep bite, and skeletal anomalies due to their inventiveness and ingenuity. The elasticity of the material and the pre-established mismatch between the aligner shape and the geometry of the dental crown, transparent aligners generate forces on the teeth and place them in the correct position [9]. Nevertheless, depending on the gravity of the case and the type of movement to be achieved, the teeth may not follow the intended or wanted movement however, the forces generated by aligners are similar to those generated by fixed appliances [7, 10]. The Movement predictability with clear aligners is significantly different, according to Rossini et al. extrusion and rotation were the most difficult movements to control (30% accuracy), contrary to upper molar distalization revealed the highest predictability (88%) [11].
In order to increase the effectiveness of orthodontic movement with clear aligner therapy, the use of auxiliaries (attachments; inter-arch elastics; mini-screws...) it is frequently recommended [11-13].
This systematic review's objectives are to determine the effectiveness of molar distalization using clear aligners and to analyze the side effects (tipping, anchoring loss, and vertical dimensions) of this treatment.
Materials and Methods
This study was registered in the PROSPERO database, under the number CRD42023438340 and followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis [14].
This systematic review included studies that met predetermined eligibility criteria, with inclusion and exclusion parameters established in accordance with the PICOS framework.
The exclusion criteria were:
Search strategy
A search of the electronic literature was conducted by two reviewers until May 2023, using Pubmed, Scoups, Science Direct, Web of Science, and EBSCO databases, without any restrictions on time or language. The search strategy included terms linked to molar distalization and clear aligner: (molar distalization or molar distal shift) and (removable thermoplastic aligners or Clear aligner OR Invisalign or Orthodontic aligner).
Study selection and data extraction
After utilizing the inclusion criteria to guide their search, two reviewers evaluated the articles based on their compliance with the inclusion criteria. Initially, they evaluated the article titles and abstracts. The complete texts of the screened articles that may be included in the review were then assessed by the same two reviewers. Articles that failed to satisfy any of the inclusion requirements were not considered for review.
Data items and collection
Study design, sample size, age, interventions, measuring material, and results means of distalization, tipping, anchorage loss, vertical dimension, and the use of elastic or attachments. All data were extracted by one author (MC) and reviewed by another author to confirm accuracy.
Risk of bias assessment
The quality evaluation was done by two reviewers, and the JBI Critical Appraisal Checklist for Quasi Experimental Studies was used to evaluate the included studies' methodological quality using the Joanna Briggs Institute's (JBI) Critical Appraisal Tools [15]. Nine items make up the checklist, which is intended to evaluate the causation of variables, baseline, control, and outcome measurement and analysis in relation to the quality of research. A "yes," "no," "unclear," or "not applicable" response is given to each item. One point is awarded if the answer is "yes." Studies that had a score of six or above were deemed high-quality and were incorporated into the review.
Results and Discussion
Study selection
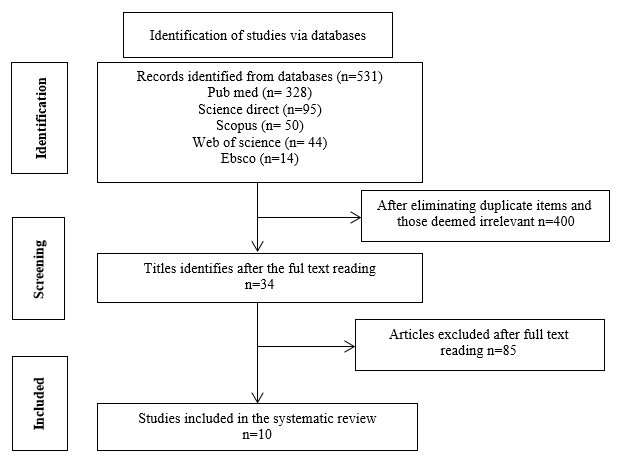
In all, the computerized search turned up 2308 references. Upon eliminating duplicates, the validity of the titles and abstracts was verified, and any articles that did not fit the selection criteria were eliminated. Ultimately, the systematic review contained 10 papers. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for the reviewing process is shown in Figure 1.
|
|
|
Figure 1. The Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) flow diagram of the reviewing process. |
In this study, ten papers that evaluated the effectiveness of molar distalization were considered. By comparing pre-treatment (T0) and post-treatment (T1) results, each included study evaluated changes in treatment outcomes. Various measurement tools were used, including digital models, lateral cephalograms, cone beam computed tomography, and digital model-integrated maxillofacial cone beam computed tomography Across the 242 patients in the listed studies, sample sizes range from 7 to 49. In every study, every patient received care without extractions (Table 1).
Table 1. Study characteristics
|
Author |
Study Design |
Simple size |
Intervention |
Measuring material |
Result |
|
Simon et al. (2014) [16] |
retrospective |
15 patients mean age 32.9 years |
Two groups of upper molars sequential distalization: 7 in group (a) with attachment, 8 in group (b) without the support of an auxiliary None of the patients used class II elastics during treatment |
the plaster casts laser-scanned |
the efficacy of upper molar Distalization was approximately 87%, irrespective of the use of an attachment. The mean accuracy of molar distalization supported with an attachment was 88.4% (SD = 0.2) Without the support of an attachment, the mean accuracy for upper molar distalization amounted to 86.9% (SD = 0.2) |
|
Cui et al. (2022) [17] |
Prospective |
18 patients with a mean age 27.8±5.38 |
upper molars sequential distalization |
Cone Beam Computed Tomography (CBCT) |
The distalization range of the U6 is 2.57±1.15mm (P<.05) and the U7 is 2.98±1.84 mm (P<.05). Aligners provided a high predictability (83.44 %) distalization of U6, and 85.14 % of U7, without obvious vertical movement or tipping (P<.05) |
|
D’Antò et al. (2023) [18] |
Prospective |
16 patients with a mean age 25.7 ± 8.8 years) |
upper molars 50% sequential distalization with the use of attachments and class II elastics |
The digital dental models |
The Overall Accuracy was 69.4% for the first molar and 75.2% for the second molar. Achieved Movement for maxillary first molar: mesio-buccal cusp MB: 1.30mm SD= 0.88 with 67.96 % accuracy Achieved Movement for maxillary second molar: mesio-buccal cusp MB: 1.76 mm SD= 1.14 with 79.89 % accuracy The aligners were not able to achieve 100% of the ideal post-treatment result; thus, planning of refinements is often needed |
|
Saif et al. (2022) [19] |
Retrospective |
38 patients with a mean age of 25.4 years |
upper molars sequential distalization without any auxiliaries other than Invisalign attachments The digital models were superimposed using the palatal rugae area for registration. |
digital models |
when a mean distalization movement of 2.6 mm was prescribed, the efficiency of maxillary molar distal movement produced by Invisalign amounted to 73.8%, where the maxillary first molar showed relatively higher efficiency (75.5%) (1.81 ±0.84) (P= 0.0001) than maxillary second molar (72.2%) (1.85 ± 0.88) (P \0.0001) No significant differences between the achieved maxillary molar distal movement with and without the use of attachments (P= 0.552) for maxillary first molar and (P=0.941) for maxillary second molar Statistically significant correlation between the amount of maxillary molar distal movement and the amount of the anterior anchorage loss. The most teeth affected by anchorage loss during molar distalization movement were central incisors (p=0.008); followed by lateral incisors (p= 0.013) |
|
Loberto et al. (2023) [20] |
Retrospective |
49 patients mean age 14.9 ± 6 years |
50% upper molars sequential distalization, with the use of Invisalign attachments and Class II elastics |
digital dental casts |
A statistically significant distalization of the maxillary molars U6 and U7, with average distalization movement of 2.5 mm U6 MB = 2.4 mm, p = 0.0001 U7 MB = 2.4 mm, p = 0.0006 Not significant anchorage loss of the first and second premolars U 4PB p= 0.5454 U5 PB p = 0.47 Statistically significant mesial movement of upper canines with average 1.33 mm. U3R C = 1.5 mm, p = 0.0001 U3L C = 1.15 mm, p = 0.008 |
|
Ravera et al. (2016) [21] |
Retrospective |
20 patients with a mean age 29.73 |
upper molars sequential distalization with the use of attachments and class II elastics. Intermaxillary elastics were used during the retraction of premolars, canines, and incisors |
lateral cephalograms |
the first molar moved distally 2.25 mm (P < 0.05) without significant tipping (P = 0.27) and vertical movements (P = 0.43). The second molar distalization was 2.52 mm (P < 0.0001) without significant tipping (P = 0.056) and vertical movements (P = 0.25). No significant movements were detected on the lower arch |
|
Lin et al. (2022) [22] |
Retrospective |
7 patients with a mean age 26.64 ± 3.02 years) |
sequential distalization of upper molars with the class II elastics |
digital model-integrated maxillofacial cone beam computed tomography |
For predicted movement between (1.36±0.82mm) and (1.98±0.62mm), treatment accuracy ranged from 31.1% to 40.1% The accuracies of distalization of the MB cusp of U6: 0.72±0.48mm; (p=0.008) with 36.5% accuracy |
|
Li et al. (2023) [23] |
retrospective |
43 patients with a mean age 28.15 ± 6.94 years |
All patients treated without extraction and divided into two groups: the retraction group (with maxillary incisor retraction ≥ sequential distalization with The attachments and Class II elastics or miniscrews were used to reinforce the anchorage |
plaster casts were collected and laser-scanned before (T0) and after treatment (T1) to obtain virtual models |
The efficacy of molar distalization with clear aligners was significantly affected by anterior teeth retraction There was a significant difference in molar distalization efficacy between the retraction group (RG) and non retraction (NRG) group (RG): At the maxillary first molar (0.78 ± 0.70 mm) p = <0.001 with efficacy 31.50% Mesiodistal (°) p=0.03 At the maxillary second molar (0.99 ± 0.97 mm) p = <0.001 with efficacy 35.63% Mesiodistal (°) p=0.006
(NRG): At the maxillary first molar (1.10 ± 1.02 mm) p = <0.001 with efficacy 48.14% Mesiodistal (°) p=0.681 At the maxillary second molar (1.29 ± 0.92mm) p = <0.001 with efficacy 52.51% Mesiodistal (°) p=0.716 |
|
WU et al. (2021) [24] |
Retrospective |
20 cases of lower molars distalization |
sequential distalizationof second and first mandibular molars |
Cone Beam Computed Tomography (CBCT) and Dolphin software |
The second and first molars were both the distal buccal cusp with the largest distalization [(2.15 ± 0.91) mm and (1.85±1.09) mm], respectively, with significant difference between the T0 and T1 (P<0.05). The second and first molars were accompanied by depression, distal tilt, and buccal tilt with 1.06 mm, 2.10°, 2.27°, and 0.91 mm, 1.62°, and 1.91°, respectively, with significant differences between the T0 and T1 (all P<0.05) The mandibular central incisor showed a lip-side movement of 1.02 mm, a depression of 0.82 mm, a mesial incline of 0.66°, and a crown-lip torque of 1.51° after molar distalization, with significant differences between the T0 and T1 (all P<0.001) |
|
Rota et al. (2022) [25] |
Retrospective |
16 patients with a mean age of 25.6 years |
sequential distalization of lower molar and premolar, with intermaxillary Class III elastics, No attachment was used during the distalization movement |
Lateral cephalometric radiographs |
the lower second molar moved distally (2.47 mm, p= 0.10) with a significant tipping (p = 0.027) the first molar, with a mean distal movement of (1.16 mm p= 0.43) and a significant tipping (p = 0.003) No significant changes were detected on the sagittal and vertical skeletal variables |
Risk of bias for individual studies
An evaluation of the quasi-experimental investigations of the JBI (Table 2).
Table 2. The JBI critical appraisal for the quasi-experimental studies
|
Checklist questions |
Q1 |
Q2 |
Q3 |
Q4 |
Q5 |
Q6 |
Q7 |
Q8 |
Q9 |
% YES |
RISK |
|
Simon et al. (2014) [16] |
Y |
Y |
N |
N |
Y |
Y |
Y |
Y |
N |
60% |
Moderate |
|
Cui et al. (2022) [17] |
Y |
Y |
Y |
N |
Y |
Y |
Y |
Y |
Y |
80% |
Low |
|
D’Antò et al. (2023) [18] |
Y |
Y |
Y |
N |
Y |
Y |
Y |
Y |
Y |
80% |
Low |
|
Saif et al. (2022) [19] |
Y |
Y |
Y |
N |
Y |
Y |
Y |
Y |
Y |
80% |
Low |
|
Loberto et al. (2023) [20] |
Y |
Y |
Y |
N |
Y |
Y |
Y |
Y |
Y |
80% |
Low |
|
Ravera et al. (2016) [21] |
Y |
Y |
Y |
N |
Y |
Y |
Y |
N |
Y |
70% |
Low |
|
Lin et al. (2022) [22] |
Y |
Y |
N |
N |
Y |
Y |
Y |
Y |
NA |
60% |
Moderate |
|
Li et al. (2023) [23] |
Y |
Y |
Y |
N |
Y |
Y |
Y |
Y |
Y |
80% |
Low |
|
Wu et al. (2021) [24] |
Y |
Y |
Y |
N |
Y |
Y |
Y |
Y |
Y |
80% |
Low |
|
Rota et al. (2022) [25] |
Y |
Y |
Y |
N |
Y |
Y |
Y |
Y |
Y |
80% |
Low |
|
JBI:Joanna briggs institute |
|
|
|
|
|
|
|
|
|
|
|
Results of included studies
The study results demonstrate varying levels of predictability, certain studies indicating predictability rates reaching up to 87%; and a displacement of 2.98±1.84 mm, while other studies report just 31.1% of predictability, and a displacement of 0.72±0.48mm. Two studies evaluated distalization of the lower molars, the second and first lower molars can be moved distally up to (2.47, 1.85 mm) respectively, with significant tipping.
In terms of tipping movement, for upper molars, the studies have shown that distalization of upper molars with aligners is practically transverse, with no significant tipping [26-31].
Two studies evaluated the reaction of distalization on anchoring units, they found that the first and second premolar anchoring loss was not considered to be significant (p=0.54; p=0.47) respectively, while a mesial displacement of the upper canines with average of (1.33 mm) which was statistically significant, was highlighted. But central and lateral incisors remain the most affected by anchorage loss (p=0.008, p= 0.013) respectively. One study showed no significant change in the lower incisors during distalization of the lower molar. All studies have concluded that molar distalization with aligners is performed with good vertical control, for first and second molar [32].
Two studies compared distalization with and without attachments and found that the efficacy of upper molar distalization was approximately similar.
The aesthetic requirements of patients are increasingly being recommended, and treatment with clear aligners meets these aesthetic demands. The goal of this research is to determine whether using clear aligners to treat complicated malocclusions is effective, thereby expanding the indications for their usage. This comprehensive review made an effort to use CA to compile the body of knowledge on molar distalization. Although molar distalization is one of the most difficult movements to achieve with conventional orthodontic treatment, it has been reported that it is one of the most predictable movement when using clear aligners [27, 33-44].
The current systematic review highlights a wide range in the predictability of molar distalization movement. Simon et al., Cui et al., Antò et al., and Saif et al. reported high accuracy rates for maxillary molar distalization, reaching up to 87%, 85.14%, 75.2%, and 75.5%, respectively, with displacement measures up to 2.98±1.84 mm [16-19]. However, these conclusions were not shared by the investigations of Lin et al. and Li et al. [22, 23]. Only 36.48% and 41.94%, respectively, of the maxillary first and second molars' predictability rates were shown by Li et al.'s investigation [23]. The maxillary first and second molars' attained molar distalization was 0.88 mm and 1.11 mm, respectively. Lin et al.’s investigation revealed a treatment accuracy ranging from 31.1% to 40.1%, coupled with a displacement of 0.72±0.48 mm at the maxillary first molar [22].
According to Li et al. the anterior tooth retraction had a major impact on the efficacy of molar distalization with clear aligners, they found the predictability in the retraction group was no more than 36% [23]. This outcome can be explained by the fact that the aligners in the retraction group were shorter to retract the anterior teeth following molar distalization. The maxillary molars underwent mesial migration as a result of aligners producing a mesial push toward them concurrently with a reduction in aligner length. But in the group that did not retract, the space made available by the molar distalization was used to relieve crowding. The distalized molars' anchoring loss was significantly decreased because the aligners' length was maintained and mesial force toward the maxillary molars was created to a low extent. In the research projects conducted by Loberto et al., Saif et al., Antò et al. and Simon et al. as soon as the first and second molars distalized, the effectiveness of molar distalization was evaluated [16, 18-20]. Nevertheless, the anchoring loss of distalized molars was ignored, as the anchorage lost in the posterior region during the retrusion of front teeth was not taken into account. This method differs from the research done by Li et al. and Lin et al. where effectiveness was assessed following the completion of the therapy while taking the anchoring loss of posterior teeth during the retraction of anterior teeth into consideration [22, 23].
Using lateral cephalograms, molar motions were evaluated in the research conducted by Ravera et al. [21]. At some point, the measurements obtained from the cephalometric and virtual model analyses differed. The post-treatment cephalometric tracing seemed to be positioned more distally and superiorly than the pre-treatment cephalometric tracing in the image showing the cephalometric superimposition by Ravera et al. [21]. That study may have overestimated the degree of molar distalization, and there is a strong chance of superimposition error. A lateral cephalogram cannot be placed on top of the anticipated virtual tooth movement, which is another limitation of the cephalometric technique.
However, in the study carried out by Cui et al. used the Cone Beam Computed Tomography after the overall treatment to assess molar distalization [17], they found that the first and second molar revealed a translation movement with a high predictability (83.44 %) for the maxillary first molar, and 85.14 % for the maxillary second molar, following a retraction of 1.40 mm of the upper incisor (U1). This raises doubts about the correlation between anterior sector retraction and molar distalization [45-53].
In order to improve the predictability of molar distalization, the attachments are used to create a moment, counteracting dental tipping, so that a vertical rectangular attachment must be designed to generate a force couple against the mesial tipping during the molar distalization [54]. According to Garino et al. the existence of attachments not only influences the distalization phase, but also contributes significantly to the anterior retraction phase, by optimizing posterior anchorage [55]. However, the effectiveness of attachments is still questionable, as indicated the studies carried out by Simon et al. and Saif et al. there was no statistically significant difference between the group with and without attachments [16, 19].
The distalization of lower molars has been the subject of only two studies [24, 25] with concordant results, the largest distalization of the second and first molars was (2.15-2.47) mm and (1.85-1.16) mm). According to the results of the two studies, this is mostly a tipping action rather than a bodily movement. In terms of tipping movement, for upper molars, the studies have shown that distalization of upper molars with aligners is practically transverse, with no significant tipping. Unlike the study by Li et al. [23], which found 2.84° of buccal tipping.
The majority of the studies have shown that the distalization of the second molar is more effective than that of the first molar, for both mandibular and maxillary molars. This could be attributed to several factors. The mechanical stimulus generated by aligners is evenly distributed among the teeth and all through the periodontal ligament; the periodontal ligament area of maxillary first molars tends to be larger than that of maxillary second molars, necessitating greater resistance to movement. Moreover, the molar distalization method utilized, where the second molar has a separate distalization process while movement of the first molar is inevitably associated with the movement of other teeth. Consequently, the amount of anchorage force required during movement varies [17].
In terms of biomechanics, during distalization, a posterior force is given to the molars and an equal and opposite reciprocal force is applied to the anterior teeth, particularly in the incisor area. This results in the loss of anterior anchoring and flaring of the incisors. After superimposing the digital models using the palatal rugae area for registration, Saif et al. saw that the central incisors (39.9%) and lateral incisors (37.4%) were the teeth most affected by anchorage loss during molar distalization movement, with canines (22.7%) being less affected [19]. Loberto et al. reported that the anchorage loss at the first and second premolars is not significant [20]. Even though patients who did not comply with using Class II elastics were aware that the study conducted by Saif et al. did not employ the elastic, a significant loss of anchoring was nevertheless found in these patients. According to this, using Class II full-time elastics was able to offset the negative effects, reinforce the anterior anchoring, and aid in the distalization movement in the anterior sector by producing an equal and opposing force to the response force [20]. The use of class II elastics during maxillary molar distalization with aligners provides appropriate control of both upper incisor extrusion and inclination, and it prevents the lower incisors from proclinating as a result of the class II elastics, as validated by Rongo et al. [56]. Furthermore, class III elastics confirm this.
When considering molar distalization, vertical dimension is a crucial consideration, particularly in individuals who are hyperdivergent. In actuality, an anterior open bite and a worsening of the profile might result from the jaw rotating clockwise due to dental precontacts that developed during the distalization process [57, 58].
Several studies have documented that the use of clear aligners resulted in improved occlusal plane control and excellent control of vertical dimension during molar distalization [17, 21, 25]. The observed outcomes might be interpreted as a consequence of reduced molar tipping during distalization, as well as lower and upper molar extrusion caused by the material covering and long-term wear. As a matter of fact, it is feasible to link an invasive force vector that can regulate any extrusion with the distalization motions while programming them, which enhances aligner fit and encourages the dental parts' natural movement [17].
Limitations
Conclusion
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None