The purpose of this study is to examine and compare the amount of external apical root resorption (EARR) in incisors observed after orthodontic treatment using fixed orthodontic appliances (FOA) or clear aligners (CAT). The systematic review was carried out adhering to PRISMA guidelines. The review included retrospective studies and randomized control trials, which performed 2D panoramic radiographs, periapical radiographs, and cone beam computed tomography to evaluate EARR levels in anterior teeth after orthodontic treatment with CAT and FOA. The focused question for the review was raised using the PICO model: does CAT induce lower levels of EARR compared to fixed orthodontic appliances The review was comprised of six articles. Five of the included publications were retrospective cohort studies and one was a randomized clinical trial. Meta-analysis revealed that CAT had a lower amount of EARR than FOA (SMD = 0.76, 95% CI = -1.17, -0.34; p<0.00001). The subgroup analysis concluded that EARR was statistically significantly lower in maxillary central incisors. (SMD = -0.40, 95% CI = -0.70, -0.10; p = 0.009), maxillary lateral incisors (SMD = -0.65, 95% CI = -0.98, -0.32; p = 0.0001) and in mandibular central incisors (SMD = -0.40, 95% CI = -0.65, -0.16; p = 0.001). Based on this meta-analysis, CAT appears to be superior to FOA in terms of EARR in the anterior teeth region.
Introduction
Since clear aligner therapy (CAT) has been introduced as a treatment method, an increasing number of patients are opting for this more esthetical and comfortable alternative treatment modality, rather than fixed orthodontic appliances. Theoretically, from the mechanical point of view, clear aligners differ from fixed orthodontic appliances in the number of orthodontic forces applied to teeth [1]. Studies have shown that orthodontic forces have a significant effect on the development of external apical root resorption (EARR) [2]. Even to this day, the exact nature of orthodontically induced root resorption remains unclear [3]. It is known that this phenomenon presents with multifactorial etiology. Patient-related (age, gender, genetics, nutrition) or treatment-related factors (the amount of force used during treatment, duration of the treatment, the type of appliance, use of elastics, extraction treatment, etc.) have contributing effects on root resorption [4]. It has also been demonstrated that heavy orthodontic forces produced significantly higher levels of EARR than light forces [3]. Therefore, heavy orthodontic forces generated by orthodontic appliances are reported as a clear cause of EARR by numerous scientific articles [5-7].
EARR is a common inflammatory response, encountered during treatment using fixed orthodontic appliances with 27,7% of cases [5]. The process is associated with the elimination of the hyalinization zone triggered by microphage-like cells from periodontal ligament blood vessels which expose the cementum and accelerate root resorption [3]. Studies have shown that the maxillary incisors are more susceptible to EARR than other teeth, due to the longer distance of orthodontic tooth movement [8]. Forces applied to the teeth by aligners are intermittent whereas during treatment with fixed orthodontic appliances forces are produced continuously. In addition, the magnitude of forces applied to the teeth by aligners is lower than by fixed orthodontic appliances [9]. These characteristics could have an impact on EARR as they cause stress in the radicular-apical area [10]. An orthodontist must assess root resorption in patients undergoing orthodontic treatment [11]. Several studies have examined EARR during CAT, however, the results are controversial – while some report decreased EARR in CAT compared to fixed orthodontic appliances, others show that CAT could lead to increased EARR [4, 9, 12-16]. Panoramic, periapical radiographs or cone-beam computed tomography is used to calculate the root-crown ratio and evaluate the longevity of the teeth [17].
The purpose of this meta-analysis was to update the current literature and compare the severity of EARR during treatment with clear aligners and fixed orthodontic appliances.
Materials and Methods
Protocol and registration
This systematic review was prepared to adhere to PRISMA guidelines. The protocol for the systematic review was registered in the PROSPERO (International Prospective Register of Systematic Reviews) database. Registration number: CRD42021240269.
Focused question
The question was raised using the PICOS model:
Does clear aligner therapy induce lower levels of external apical root resorption compared to fixed orthodontic appliances?
Search strategy
On November 6, 2022, a systematic search in the medical literature was carried out to identify all peer-reviewed papers, published from 2016 to 2022, evaluating the amount of EARR in patients who received CAT or treatment with fixed orthodontic appliances. Combinations of keywords “Clear Aligner Appliances”, “Fixed Orthodontic Appliances”, and” Root resorption” were used in MEDLINE (searched via PubMed), EMBASE (searched via ScienceDirect), System for Information on Grey Literature in Europe, The Cochrane Library (Cochrane Central Register of Controlled Trials) and LILACS electronic bibliographic databases. Furthermore, the search was broadened by checking for possible articles in the references of the included articles.
Study selection and data collection process
Three authors (K.J., M.V., and A.Var.) performed an electronic database search and selected articles that appeared to have appropriate titles and abstracts for the review and met the criteria. After reviewing the full-text articles, the final selection was made. The fourth reviewer (A.Vas.) would have tried to resolve the conflict, if there were any discrepancies.
Inclusion criteria
Exclusion criteria
Methodological quality
The Cochrane Collaboration's ROBINS-I tool [18] and the Cochrane risk-of-bias tool for randomized trials (RoB 2) were used to assess the overall quality and risk of bias in this systematic review, evaluating confounding, study participant selection, intervention classifications, deviation from intended interventions, missing data, outcome measurement, and reported result selection.
Statistical analysis
To perform meta-analysis, the means, standard deviations, and sizes of study samples were extracted. An inverse variance method with random effect model meta-analysis was conducted to compare the standard mean difference (SMD) in EARR between patients who received fixed orthodontic appliance therapy and clear aligner therapy with a 95% confidence interval (CI). Cochran’s Q and I2 tests were used to evaluate the heterogeneity of the studies. The heterogeneity was considered to be significant when P<0,05 for Q statistics or I2>50%. Summarized quantitative data were graphically presented in forest plots using Review Manager 5.4.1 software [19]. Sensitivity analysis was conducted to test the stability of the results, and whether the exclusion of some studies had any impact on the outcome of the results.
Results and Discussion
Study selection
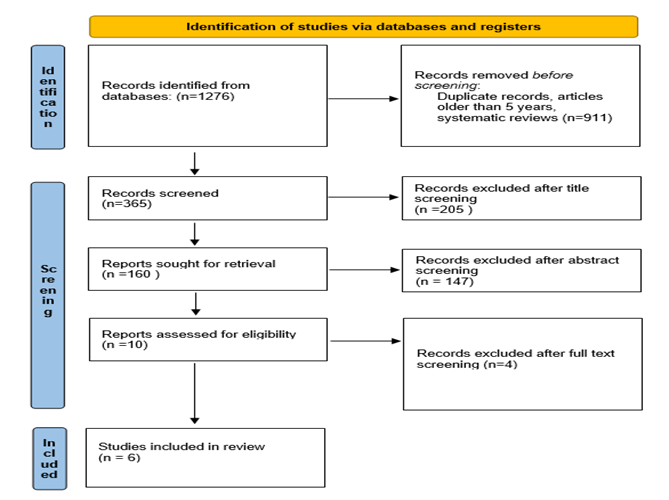
The procedure of study selection is presented in Figure 1. The initial electronic database search yielded 1276 articles. After removing the articles that were not relevant based on their title and abstracts, ten full-text papers were retrieved and reviewed for their suitability. Four studies were excluded for the following reasons: two studies were excluded because they were theses [20, 21], one study was considered not suitable as it was a case-control genetic association study [22], and another study was excluded since it was published in Mandarin [23]. Hence, 6 publications [9, 12, 14, 16, 24, 25], were included in the qualitative and quantitative data analysis.
Study characteristics
Table 1 presents characteristics of all 6 articles that were included in the review. 5 of the included publications were retrospective cohort studies and 1 was a randomized clinical trial. The publication dates of the articles were between the years 2017 and 2022. Several patients ranged from 33 to 110 (a total of 391 patients were included in all 6 studies) with ages ranging from 14 to 31 years. Treatment duration did not significantly differ between different treatment modalities. All of the included studies compared clear aligner therapy with fixed orthodontic appliances. Two studies compared clear aligners with two different types of fixed orthodontic appliances [12, 25]. All 6 publications evaluated maxillary incisors, and four of them assessed mandibular incisors [9, 14, 16, 24]. Two studies evaluated canines additionally [14, 16]. Four studies assessed EARR by using CBCT [9, 12, 16, 25], one study performed measurements using a 2D panoramic radiograph [14] and one study performed measurements using a 2D periapical radiograph [24].
Table 1. General characteristics of the selected studies
|
|
Study |
Study type |
Participants (sample size) |
Intervention (type of appliance) |
Participants (mean age, years (SD)) |
Participants (gender) |
Evaluation method |
Evaluated teeth |
Outcome (root resorption) |
|
1 |
Eissa, 2018 [12] |
Retrospective |
33 patients |
G1:Smart Track® aligners, G2: Damon‐Q self‐ligating brackets, G3:Regular preadjusted edgewise brackets |
G1: 18.34 (2.82) G2: 17.71 (2.22) G3:17.34 (2.38) |
G1: 5 males, 6 females G2: 4 males, 7 females G3: 6 males, 5 females |
CBCT |
Maxillary central incisors,maxillary lateral incisors |
G1: 0.44±0.35mm, G2: 0.55±0.38mm, G3: 1.04±0.67mm |
|
2 |
Li, 2020 [14] |
Retrospective |
70 patients |
G1: Invisalign clear aligners, G2: Conventional fixed orthodontic appliances (Victory Series) |
G1: 24.71 (7.48) G2: 2.51 (6.47) |
G1: 13 males, 22 females G2: 8 males, 27 females |
CBCT |
Maxillary and mandibular central and lateral incisors, maxillary and mandibular canines (total 373 teeth) |
G1: 0.13 ±0.47mm G2: 1.12 ± 1.34mm |
|
3 |
Yi, 2017 [9] |
Retrospective |
80 patients |
G1: Clear aligner therapy (sequential thermoplastic appliances) G2: Fixed orthodontic appliances (preadjusted edgewise appliance) |
G1: 21.80 (5.11) G2: 23.28 (5.60) |
G1: 31 females, 9 males G2: 29 females, 11 males |
Digital panoramic radiographs |
Maxillary and mandibular central and lateral incisors (total 640 teeth) |
G1: 5.13 ± 2.81%, G2: 6.97 ± 3.67% |
|
4 |
Jyotirmay 2021 [16] |
Retrospective |
110 patients |
G1: Fixed appliances (3M, USA) G2: Clear aligners |
G1: 23.71 (6.37) G2: 21.62 (3.58) |
G1: 32 females, 23 males G2: 34 females, 21 males |
CBCT |
Maxillary and mandibular central and lateral incisors, maxillary and mandibular canines (total 576 teeth) |
G1: 1.51 ±1.34 mm G2: 1.12 ±2.36 mm |
|
5 |
Toyokawa- Sperandio 2021 [24] |
Randomized clinical trial |
39 patients |
G1: OAs (SmartTrack, InvisalignTM; Align Technology, San Jose, CA, USA). G2: Fixed metallic orthodontic appliance (slot 0.022” × 0.030”, 3M Unitek, Monrovia, CA, USA) |
G1: 23.60 (5.65) G2: 20.56 (4.51) |
G1: 8 females, 12 males G2: 7 females, 13 males |
Periapical radiographs |
Maxillary and mandibular incisors (total 312 teeth) |
G1: 0.66 ±0.19 mm G2: 0.73 ±0.21 mm |
|
6 |
Chen, 2022 [25] |
Retrospective |
59 patients |
G1: fixed orthodontic appliances with 0.022-in slot (Victory Series; 3M Unitek, Calif). G2: Damon Q with a 0.022-in slot (DQ; Ormco, Orange, Calif). G3: Aligners (Invisalign, Align Technology, Calif) |
G1: 23.60 (3.19) G2: 23.71 (3.44) G3: 22.67 (3.12) |
G1: 11 females, 9 males G2: 13 females, 8 males G3: 12 females, 6 males |
CBCT |
Maxillary central incisors |
G1: 0.87 ±1.08 mm G2: 0.94 ±1.41 mm G3: 0.92 ±0.87 mm |
Note. G – treatment group, SD – standard deviation, %= percentage, CBCT – cone beam computed tomography
Quality assessment
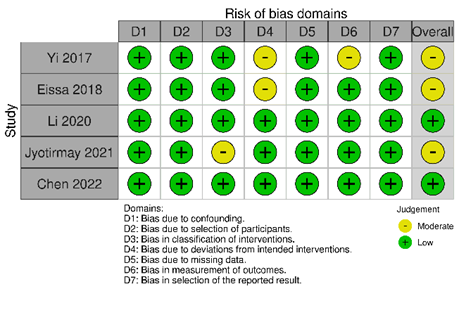
By the ROBINS-I tool, all five publications had a low risk of confounding, participant selection, missing data, and reported results selection bias. Two out of five studies had moderate bias due to deviations from intended interventions [9, 12], one had a moderate risk of measurement of outcomes [9] and one had a moderate risk classification on intervention bias [16]. Two studies had a low risk of bias for all of the analyzed factors [14, 25]. According to the Cochrane risk-of-bias tool for randomized trials (RoB 2), one study had a moderate risk of bias in blinding participants and personnel [24]. Overall, three studies had moderate [9, 12, 16], and three had low risk of bias [14, 24, 25] (Figure 2).
|
|
|
a) |
|
|
|
b) |
|
Figure 2. Quality assessment |
Quantitative synthesis of the results
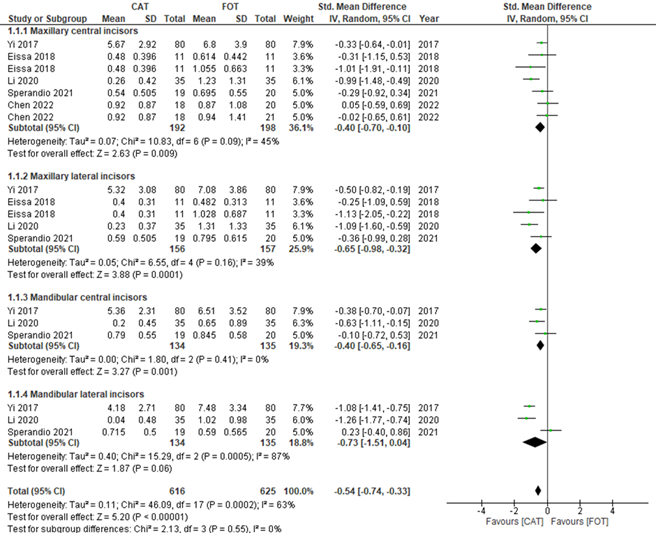
When the EARR data was evaluated, it was observed that, even with different scales, the CAT significantly benefited this outcome (SMD = 0.76, 95% CI = -1.17, -0.34; p < 0.00001). However, due to the significant heterogeneity among studies (p = 0.004, I2 = 60%), subgroup analyses depending on the group of the teeth (maxillary central incisors, maxillary lateral incisors, mandibular central incisors, and mandibular lateral incisors) were performed (Figure 3).
|
|
|
Figure 3. Quantitative subgroup analysis |
EARR in maxillary central incisors
Five studies evaluated EARR in maxillary central incisors [9, 12, 14, 24, 25]. No significant differences in heterogeneity were found among studies (p = 0.09, I2 = 45%) and meta-analysis demonstrated that CAT has a lower quantity of EARR (SMD = -0.40, 95% CI = -0.70, -0.10; p = 0.009). The sensitivity analysis showed that the removal of any particular studies from the meta-analysis does not modify the outcome significantly
EARR in maxillary lateral incisors
Four studies evaluated EARR in maxillary lateral incisors [9, 12, 14, 24]. No significant differences in heterogeneity were found among studies (p = 0.16, I2 = 39%) and meta-analysis demonstrated that CAT has a lower quantity of EARR (SMD = -0.65, 95% CI = -0.98, -0.32; p = 0.0001). The sensitivity analysis showed that the removal of any particular studies from the meta-analysis does not modify the outcome significantly.
EARR in mandibular central incisors
Three studies evaluated EARR in maxillary central incisors [9, 14, 24]. No significant differences in heterogeneity were found among studies (p = 0.41, I2 = 0%) and meta-analysis demonstrated that CAT has a lower quantity of EARR (SMD = -0.40, 95% CI = -0.65, -0.16; p = 0.001). The sensitivity analysis showed that the removal of any particular studies from the meta-analysis does not modify the outcome significantly.
EARR in mandibular lateral incisors
Three studies evaluated EARR in mandibular central incisors [9, 14, 24]. Significant differences in heterogeneity were found among studies (p = 0.0005, I2 = 87%) and meta-analysis demonstrated that CAT has a lower quantity of EARR (SMD = -0.73, 95% CI = -1.51, -0.04; p=0.06). The sensitivity analysis showed that the removal of the study by Toyokawa-Sperandio et al. [24] from the meta-analysis does change the outcome significantly. Without that study, no significant differences in heterogeneity were found among studies (p = 0.57, I2 = 0%) and meta-analysis demonstrated that CAT has a lower quantity of EARR (SMD = -1.13, 95% CI = -1.41, -0.85; p < 0.00001
Discussion
The main purpose of this systematic review was to analyze the current literature and compare the EARR incidence in maxillary and mandibular incisors during CAT and FOAT. However, due to a limited number of publications that compared clear aligners and fixed orthodontic appliances in the same study was low, we were limited solely to retrospective studies and one randomized clinical trial. Nevertheless, a meta-analysis was performed, and its results showed that clear aligner therapy exhibits significantly lower levels of EARR.
Even though the results of the meta-analysis showed that EARR incidence in the CAT group was lower, such treatment modality is still not an exception for EARR. According to Li et al. study, 56.3% of patients in the CAT group experience EARR at least on a single tooth [14]. However, according to Sharpe’s method of defining the severity of root resorption [26], all of the EARR incidents appear to have just a 1° EARR, while 20.05% of the patients in the fixed orthodontic appliances therapy (FOAT) group experience 2° or 3° root resorption, indicating that the amount and severity of the EARR in FOAT group is far more advanced. Moreover, a study by Eissa et al. evaluated EARR incidence between Damon brackets and pre-adjusted edgewise brackets [12]. No significant differences were found. Similarly, trials by Aras et al., Liu et al. and Chen et al. could not prove the superiority of a particular kind of fixed orthodontic appliance over any other, regarding EARR [23, 27, 28].
Four studies included in this systematic review used CBCT to evaluate EARR incidence [9, 12, 16, 25], one study performed measurement using 2D periapical radiograph [24], while 1 study used 2D panoramic radiograph [14]. CBCT is superior to 2D panoramic radiographs as it provides three-dimensional data, enabling a doctor to examine root resorption at both, lingual and buccal sides. CBCT, therefore, enables clinicians to measure close-to-exact EARR. The meta-analysis performed by Ghandi et al. revealed that the amount of EARR found with 2D methods was about 0.2 mm higher compared to 3D methods, due to 2D radiographs known characteristic of magnifying and distorting images, especially in the anterior teeth region [4]. The sensitivity analysis revealed no significant differences when excluding the study by Yi et al. which incorporated a 2D radiograph as a means to evaluate EARR. The reason might be adopting the results as relative root-crown ratio changes, rather than absolute values. Except for a small number of patients who grind their incisors, tooth crown lengths remain nearly constant following orthodontic treatment, and the accuracy of the relative change in the root-crown ratio may be acceptable despite variations in distortion and magnification between the panoramic radiographs taken before and after the treatment.
A former systematic review published by Gandhi et al. in 2020 included randomized clinical trials and retrospective studies from 2009 to 2019 [4]. Our review includes the newest articles from 2017 to 2022. Gandhi et al. reported no significant difference in EARR between CAT and treatment with fixed orthodontic appliances whereas our study showed that EARR is more prevalent in the fixed orthodontic appliances group.
Although the precise mechanism of EARR remains unclear, it is believed that EARR has a direct connection to orthodontic forces and apical movement distance [1, 8]. From a mechanical point of view, orthodontic forces delivered to teeth through CAT are intermittent, while in FOAT they are continuous [9]. In the study by Aras et al. it was observed that teeth exposed to continuous orthodontic forces are subjected to a higher prevalence of EARR compared to intermittent ones [27]. An explanation for this phenomenon is that the cementum, subjected to intermittent forces has time to heal, especially keeping in mind that patients with clear aligners usually remove them while eating or performing daily oral health care. Several studies examined EARR dependence on the duration and intensity of the force applications, concluding that the magnitudes of the forces were connected to the volumes of root resorption craters [2, 3, 8]. The included studies evaluated demographical and clinical information, and risk factors such as patients’ sex, age, skeletal pattern, treatment duration, extraction and non-extraction cases, malocclusion type, and crowding severity. However, none of the mentioned subjects were considered statistically significant contributory factors for EARR in the previous publications. Considering the limitations of this meta-analysis, the sample of currently available studies is not extensive, which, in turn, leads to deficient statistical power. Moreover, even though statistical heterogeneity was not recorded, clinical heterogeneity could be deducted due to several reasons. Firstly, one of the included studies evaluated EARR by using a percentage of the root resorption, while others measured it by millimeters. Secondly, one study adopted a 2D panoramic radiograph to measure EARR and one used 2D periapical radiographs, while others - CBCT.
Conclusion
Based on the current meta-analysis, we conclude that in terms of the quantity of EARR in the anterior tooth region, CAT is generally preferable to fixed orthodontic appliances. These findings should be interpreted cautiously, though, as further methodologically sound clinical trials are required to offer more conclusive proof.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None