The ideal way to describe minimal invasive dentistry is to treat caries using a biological strategy as opposed to a conventional (surgical) operational dentistry strategy. In cases when surgical dentistry is necessary, treatment is now done as conservatively as possible, causing the least amount of damage to the tooth's structure. This novel method of managing carious lesions shifts the focus from identifying the lesions as cavities (and a recurring cycle of restorations) to identifying the ecological imbalance in the mouth and bringing about biological changes in the biofilm. Minimally Invasive Dentistry (MI) aims to maximize the tooth's ability to recover by first halting the disease process and then restoring lost tooth structure and function. Dietary and lifestyle choices, particularly those involving the frequency of carbohydrates, water consumption, and smoking, have a significant impact on the pathogenicity and ecology of biofilms. Chairside tools for measuring plaque and saliva enable risk to be evaluated and patient compliance to be tracked. Materials that release physiologically accessible calcium, phosphate, and fluoride ions (CPP-ACP and CPP-ACFP) may improve saliva's remineralizing qualities. The use of biocides may also change the pathogenic qualities of plaque. By using these MI therapy methods, early lesions may be repaired, and patient comprehension and compliance may be increased. A few of the main ideas and useful applications of minimally invasive dentistry are covered in this review article.
Introduction
The term “Minimal Invasive” (MI) Dentistry can be defined as the management of dental caries with a biological/medical approach, as compared to traditional operative dentistry which is based on surgical and mechanical principles. It focuses on the results of the disease (cavitations) but does not address the preceding disease process. The MI approach has been developed because of the many failures associated with traditional operative dentistry. Traditional diagnosis involves detecting carious lesions at a late stage (frank cavitation) and then restoring these cavities, usually with a G.V. Black cavity preparation and the use of amalgam or composite. Unfortunately, removing the evidence of the disease does not stop the disease process from continuing at other sites. In other words, placing dental restorations does not ‘cure’ caries. No restoration can be considered permanent. In fact, unless the ongoing causes of the disease are addressed, restoration failure from recurrent caries is highly likely, and this premature failure results in ongoing restoration replacement, resulting in larger and larger cavities and weakening of tooth structure. To overcome this, the caries disease process needs to be managed in partnership with the patient and over the lifetime of the patient.
Materials and Methods
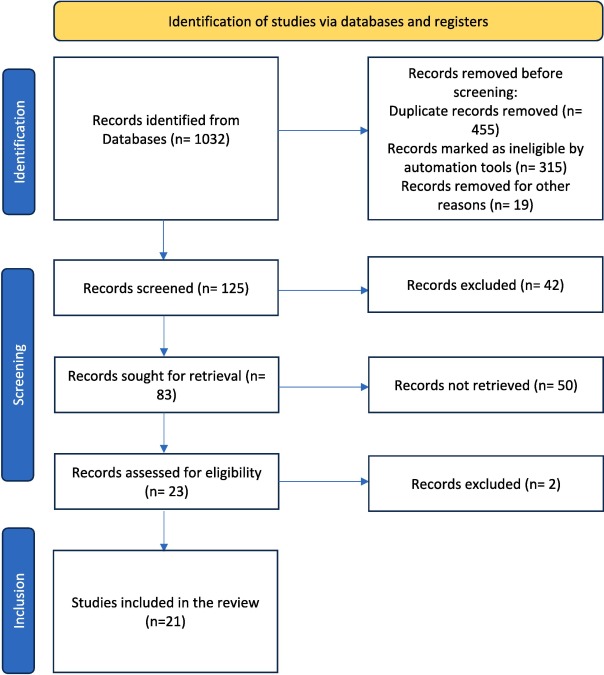
In June 2023, a search was carried out across a number of electronic databases, including PubMed, SCOPUS, EMBASE, COCHRANE Library, and Science Direct, in order to undertake a literature assessment on minimally invasive dentistry. MeSH phrases and keywords, including "minimum intervention dentistry," "atraumatic restorative treatment (ART)," "mid," and "minimum invasive dentistry", were used in the search. Cross-references and textbooks were manually searched for pertinent articles in addition to the computerized searches. Articles that met the study's goals and were published in English between 2000 and June 2023 were included. Evaluation of the inclusion and exclusion criteria, as well as a quality evaluation, were part of the article selection process. Based on their titles and abstracts, 121 of the first 1032 discovered publications were chosen. There were eighty-three items in all after a manual search turned up four more. Twenty-one papers that met the study's requirements were selected for assessment after the complete texts were assessed and the inclusion and exclusion criteria were applied. The screening method did not include narrative assessments of MID or animal experiments (Figure 1).
|
|
|
Figure 1. PRISMA flowchart to describe the screening process |
Results and Discussion
New developments in minimally invasive methods
Micro-wearing
This method of removing superficial enamel flaws and discolorations is less intrusive. Using a high-speed handpiece and a mixture of mild abrasive substances, the exterior enamel layer is mechanically abraded [1, 2]. Fluorosis stains, minor enamel hypoplasia, and white or brown demineralized patches are the areas where this technique works best. When treating problematic teeth, microabrasion may greatly enhance their aesthetics without requiring invasive procedures or thorough tooth preparation. To get the best outcomes, it is often used in conjunction with other minimally invasive procedures, such as enamel bonding or bleaching [3, 4].
Infiltration of resin
Resin infiltration is a minimally invasive treatment that stops the progression of early caries by infiltrating a low-viscosity resin into the porous enamel structure. This effectively prevents the lesion from getting worse and improves the tooth's appearance. The resin infiltrant fills the voids in the enamel, strengthening its structural integrity and covering up the discoloration left by carious lesions. Resin infiltration is frequently combined with other minimally invasive therapeutic techniques to provide comprehensive care for dental caries [5].
Bleaching
One popular least invasive method for treating tooth discoloration and improving smile aesthetics is teeth whitening. Bleaching chemicals like hydrogen peroxide or carbamide peroxide are used to eliminate intrinsic and extrinsic stains from the tooth structure. Bleaching may be done at home using specially-made trays and bleaching gels, or it can be done in the office under the guidance of a professional. Without requiring intrusive treatments, this method works well for enhancing the brightness and hue of teeth. Patients who have discolored teeth due to aging, tobacco use, or certain dietary patterns would benefit most from it. In order to get complete outcomes, bleaching may be coupled with other minimally invasive treatments, such as microabrasion or composite resin restorations. Bleaching provides a conservative and affordable way to improve smile aesthetics [6].
Computer-aided design/computer-aided manufacturing (CAD/CAM) technology with digital dentistry
The exact manufacture of restorations made possible by CAD/CAM eliminates the need for conventional impressions and makes minimally invasive treatment planning easier [7, 8].
Biomimetic strategies
With materials and methods that closely approximate natural tooth features, biomimetic dentistry seeks to replicate the structure and function of teeth in order to improve lifespan and aesthetics [9].
Methods using a laser
Dental lasers provide accurate, less invasive treatment alternatives for a range of treatments, including tooth whitening, soft tissue management, and cavity preparation [10].
Nanotechnology in materials for restoration
With just minimum tooth preparation required, stronger and more aesthetically pleasing restorations may be created because of nanomaterials' enhanced mechanical and physical qualities [11].
Recent developments in minimally invasive dentistry are bringing more effective, patient-centered, and long-lasting treatment alternatives to the field of restorative dentistry.
Clinical instances and proof of minimally invasive methods
Clinical significance of minimally invasive procedures
Clinical justifications for minimally invasive restorative dental treatments are many. They are useful in treating several ailments, such as:
Moderate-to-small carious lesions
For the conservative treatment of small-to-moderate-sized cavities, less invasive methods such as composite resin restorations are ideal because they preserve as much of the good tooth structure as possible [12, 13].
Nanotechnology in dentistry, Resin Infiltration Bleaching, Biomimetic approach, and microfabrasion laser-aided procedures.
Wear on teeth
In order to minimize tooth preparation and address both functional and aesthetic issues, minimally invasive techniques may successfully replace teeth that have been impacted by attrition, abrasion, or erosion [14].
Flaws and discolorations in enamel
Veneers and bonding are two common techniques used to cover discoloration and repair enamel flaws, including enamel hypoplasia or fluorosis, giving the teeth a more aesthetic look [15].
Chipped or broken teeth
Adhesive bonding and composite resin materials are used in minimally invasive treatments to restore chipped or broken teeth in a way that looks and functions natural [16].
Prolonged clinical results and success ratios
The success rates and long-term clinical results of minimally invasive therapeutic dental procedures have been the subject of numerous research [17, 18]. Positive outcomes have been frequently seen in these trials. Ceramic inlays and onlays, for instance, show exceptional endurance and clinical performance. Long-term follow-up studies on composite resin restorations, for example, have demonstrated great survival rates, with success rates ranging from 80% to 95% after 5 years to 10 years. After ten years, long-term trials have shown survival rates of around 90% with few problems or failures [19].
Furthermore, veneer and bonding methods have shown good long-term results, with little repair failure and great patient satisfaction. The lifespan and effectiveness of minimally invasive restorations are largely dependent on careful case selection, precise adhesive bonding, and routine maintenance.
Patient acceptance and satisfaction
An important criterion for assessing the effectiveness of minimally invasive procedures is patient acceptance and satisfaction. Numerous investigations have shown elevated degrees of patient contentment and adoption of these methodologies [20]. Patients like that their natural tooth structure is preserved, that the treatments are less intrusive, and that tooth-colored restorations enhance aesthetics. Comparing minimally invasive therapies to older methods, they also often lead to less postoperative sensitivity and pain. Higher levels of satisfaction result from shorter treatment periods, less anesthesia required, and quicker recovery for patients [21].
Studies that compare with conventional methods
Research has been done to compare the benefits and efficacy of minimally invasive procedures to those of conventional methods. These studies have repeatedly shown that minimally invasive procedures have significant advantages over standard methods and provide results that are on par with or better than them. Studies contrasting composite resin restorations with conventional amalgam restorations, for instance, have shown that composite resin restorations have comparable or superior lifespan, better aesthetics, and a lower risk of tooth breakage. Research has shown that ceramic restorations provide better lifespan, biocompatibility, and aesthetics than conventional metal-based restorations. Studies comparing the effectiveness of less invasive veneers and bonding methods to more invasive treatments like complete crowns or significant tooth preparation have shown positive effects [22, 23].
Challenges and Limitations of Minimally Invasive Procedures in Restorative Dentistry: Despite the many benefits that minimally invasive procedures in restorative dentistry provide, there are a few issues and restrictions that need to be taken into account. Dentists need to comprehend these difficulties in order to provide appropriate and successful patient treatment.
Recent developments in minimally invasive dentistry have revolutionized the discipline by providing more effective, patient-centered, and long-lasting treatment choices. Now, let us explore the topic and contrast these developments with earlier research.
Microabrasion has become a useful technique for treating minor flaws and discolorations in the enamel. Research demonstrating its efficacy in treating demineralized spots, fluorosis stains, and moderate enamel hypoplasia, including that conducted by Rayapudi and Usha (2018) [24]. This method is unique in that it may improve tooth appearance without requiring intrusive procedures. Microabrasion offers a less invasive option with better results than previous methods, eliminating the need for significant tooth preparation.
Resin infiltration has stopped the development of incipient carious lesions and improved their appearance, therefore revolutionizing the therapy of these diseases. It has been shown by Mirsiaghi et al. (2018) [9] to be beneficial in healing non-cavitated lesions, maintaining tooth structure, and enhancing aesthetics. In contrast to conventional restorations, resin infiltration promotes conservative treatment strategies with good long-term results by minimizing the destruction of healthy tooth tissue.
Bleaching procedures have been enhanced to treat tooth discoloration efficiently while maintaining dental integrity. According to Prabhakar et al. (2015) [25], it has advantages in terms of improving smile aesthetics without requiring invasive operations. Modern whitening techniques provide better safety, effectiveness, and patient satisfaction than older techniques, which makes them the method of choice for treating tooth discoloration.
Because digital dentistry and CAD/CAM technologies allow for exact restoration construction, treatments have become more efficient. Research by Kumar et al. (2021) [5] highlights the accuracy and efficiency of CAD/CAM systems in treatment planning. This innovation provides better results and patient comfort, and it represents a considerable shift from conventional impression techniques.
By imitating the structure of natural teeth, biomimetic techniques seek to improve both lifespan and appearance. It has been highlighted by Da Mata et al. (2015) how crucial it is to choose materials that closely mimic the characteristics of genuine teeth. By placing a higher priority on maintaining the functional integrity and structure of teeth than traditional therapeutic methods, biomimetic dentistry is a paradigm shift.
Nanotechnology and laser-assisted procedures have added even more minimally invasive alternatives to the arsenal. Their accuracy and efficacy in different dental treatments have been emphasized by Banerjee et al. [13] and Tumenas et al. (2014) [26]. These developments shorten healing times and lessen patient suffering by providing better results with less tissue damage.
Clinical applications and research show that minimally invasive procedures are versatile in treating a range of diseases, including fractures, carious lesions, tooth attrition, and enamel abnormalities. The effectiveness and dependability of these strategies have been shown by long-term research that regularly provides positive results and high patient satisfaction ratings [21, 22].
Because digital dentistry and CAD/CAM technologies allow for exact restoration construction, treatments have become more efficient. Research by Kumar et al. (2021) [5] highlights the precision and efficiency of CAD/CAM systems in treatment planning. This innovation provides better results and patient comfort, and it represents a considerable shift from conventional impression techniques.
By imitating the structure of natural teeth, biomimetic techniques seek to improve both lifespan and appearance. Nguyen et al. (2022) have highlighted how crucial it is to choose materials that closely mimic the characteristics of actual teeth [20]. By placing a higher priority on maintaining the functional integrity and structure of teeth than traditional therapeutic methods, biomimetic dentistry is a paradigm shift.
Nanotechnology and laser-assisted procedures have added even more minimally invasive alternatives to the arsenal. Their accuracy and efficacy in different dental treatments have been emphasized by Banerjee (2015) [13] and Tumenas et al. (2014) [26]. These developments shorten healing times and lessen patient suffering by providing better results with less tissue damage.
Prospects for minimally invasive dentistry techniques in the future
Prospective developments and novelties
There are various anticipated breakthroughs and advances in the rapidly developing area of minimally invasive dentistry. Among them are:
Cutting-Edge restorative materials
The goal of ongoing research is to create novel restorative materials that are more aesthetically pleasing, biocompatible, and durable. Bioactive composites and smart materials are examples of biomimetic materials that closely resemble the natural characteristics of teeth and have been investigated for possible use in minimally invasive restorations [27].
Three-dimensional (3D) printing with digital dentistry
The combination of digital dentistry and 3D printing technology presents exciting opportunities for less invasive dentistry. When paired with 3D printing, CAD and CAM technology allow for the accurate creation of restorations while also enhancing efficiency, accuracy, and customization [17].
Regenerative methods
Dental tissues that have been lost or injured may be repaired using regenerative methods, including tissue engineering and stem cell therapy. By encouraging the natural healing and regeneration of tooth structures, these methods may completely transform restorative dentistry and lessen the necessity for intrusive procedures [8].
Dentistry for implants with minimal invasion
The development of less invasive methods for implant insertion and restoration has been the main focus of advancements in implant dentistry. To maximize treatment results while reducing invasiveness, guided implant surgery, instantaneous implant loading, and novel implant materials are being investigated [20].
Research on minimally invasive techniques
The development and improvement of minimally invasive restorative dentistry depend heavily on ongoing research. The following areas should be the focus of future research.
Extended clinical research
Long-term clinical trials will provide important information on the robustness, efficacy, and patient satisfaction with minimally invasive procedures. As a result, evidence-based policies and procedures for successful implementation will be established [28].
Studies on comparative effectiveness
Comparative studies contrasting their results with those of conventional methods are necessary to prove the superiority, advantages, and economic viability of minimally invasive procedures. According to Maldupa et al. (2022) [7], these findings provide further evidence in favor of the acceptance and incorporation of minimally invasive techniques in standard clinical practice.
Material creation and examination
The creation and testing of novel materials with enhanced characteristics, durability, and aesthetics for minimally invasive restorations need to be the main emphasis of research. This entails examining how materials behave in various oral environments and evaluating their biocompatibility, robustness, and resistance to deterioration and discoloration.
Acceptance and pleasure of patients
An important criterion for assessing the effectiveness of minimally invasive procedures is patient acceptance and satisfaction. Numerous research has shown that patients are quite satisfied and embrace these methods [25, 29]. Patients like that their natural tooth structure is preserved, that the treatments are less intrusive, and that tooth-colored restorations enhance aesthetics.
Comparing minimally invasive treatments to older methods, they also often lead to less postoperative sensitivity and pain. Higher levels of satisfaction result from shorter treatment periods, less anesthesia required, and quicker recovery for patients.
Studies that compare conventional methods with studies comparing minimally invasive procedures to standard methods have been done to assess the benefits and efficacy of each [13, 14]. These studies have repeatedly shown that minimally invasive procedures have significant advantages over standard methods and provide results that are on par with or better than them. Studies contrasting composite resin restorations with conventional amalgam restorations, for instance, have shown that composite resin restorations have comparable or superior lifespan, better aesthetics, and a lower risk of tooth breakage [23, 30].
Research has shown that ceramic restorations provide better lifespan, biocompatibility, and aesthetics than conventional metal-based restorations.
Studies comparing the effectiveness of less invasive veneers and bonding methods to more invasive treatments like complete crowns or significant tooth preparation have shown positive effects.
Conclusion
In restorative dentistry, minimally invasive procedures have become a key strategy for maintaining natural tooth structure, achieving the best possible treatment results, and raising patient satisfaction. With possible developments in materials, technology, and regeneration techniques, the future of minimally invasive dentistry is bright. For these methodologies to be further refined and validated, research must go on. Research on material development, comparative efficacy, and long-term clinical trials are essential for developing evidence-based practices, improving treatment results, and broadening the scope of minimally invasive techniques. Dentists may provide patients with conservative, efficient, and patient-centered treatment by adopting the minimally invasive dentistry tenets and incorporating new developments in technology and materials. This results in better dental health, more attractive teeth, and happier patients.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None