
Prevalence of Congenitally Missing Teeth (Radiographic Study)
Hussein Haleem Jasim
Department of Oral Diagnosis, College of Dentistry, University of Wasit, Kut city, Iraq.
|
|
Introduction
Patients refer to dentists due to different problems.1 There are teeth abnormalities with different types and severities 2-4 such as extra or missing teeth, and Taurodontism.5 The congenitally missing teeth “(teeth agenesis)” are one of the abnormalities that can be occurred in one or both of the jaws which are referred to as an absence of a single tooth or multiple teeth and it may be unilateral or bilateral tooth/ or teeth missing. In general, the congenitally missing teeth interfere negatively on the dental esthetic, occlusion and the masticatory function in the individuals with this abnormality.
Various terms describe the absence of teeth as “hypodontia, oligodontia, and anodontia”.5-8 “Hypodontia” refers to the absence of up to six teeth, “oligodontia” refers to the absence of more than six teeth while “anodontia” refers to the complete absence of teeth.9 That is widely registered in different regions of the world according to many studies.10-29
Studies on this abnormality were distributed around the continents of the world. The studies in Europe, America, and Australia found 5.5% in Europe, 6.3% in Australia and lower rates were in North America.26 These anomalies are rarely associated with deciduous teeth, but their occurrence is common between the permanent teeth, some studies stated that there was a relationship between the congenitally missing teeth in both deciduous and permanent teeth. The reports stated that the occurrence of congenitally missing teeth in children was due to the loss of the corresponding successor's primary teeth.27, 28 Many studies stated that the congenitally missing teeth can be associated with some oral or other abnormalities, “microdontia” considered the most widely feature associated with cases of teeth agenesis.29
Also, other abnormalities may be associated with these cases, like cleft lip and palate, and Down ‘syndrome.6, 27, 30 The ectopic position of permanent, Peg shaped maxillary lateral incisors, enamel hypoplasia, palatal inclined or impacted maxillary canines and molar infra-occlusion.31-33 Rotations and generalized spacing of the teeth beside missing mandibular second premolars can be seen.32 As well as, over-erupted and reclined mandibular incisors which cause increase overbite can be seen.34
Etiology of congenitally missing teeth
During the early phases of tooth development, any disturbances in the early phases of this period lead to congenitally missing teeth.35 Genetics plays a major and critical role in the development of these anomalies.36 Several studies confirmed the genetic effect of researches on monozygotic twins.18, 37-39 It is reported that the absence of anterior teeth may depend mainly on genes, but the absence of posterior teeth might be controversial.40 Environmental factors have a role in the etiology of these anomalies or combination with genetic factors.
Many studies reported that the “ectoderm” undergoes “dysplastic expression” due to these factors.18, 40-42 Due to the environmental factors, the tooth germ is developing after closing the space available for the development of teeth b the surrounding tissues.20, 43 When the primary teeth are missing congenitally, their permanent analogs may also be missing.18, 44
Various genes were reported and might be responsible for the occurrence of congenitally missing teeth.45-50 Mutation of these genes (as PAX9, TGFA, and MSX) might be associated with the development of congenitally missing teeth between different ethnic groups.15, 49, 51-57 MSX1 and MSX2 have an important role as mediator for the interactions of epithelial and mesenchymal tissues during dental development. 52, 58, 59 For example, mutations in MSX1 have a direct effect on the development of second premolars and third molars and sometimes the first molar.22 But on the common incisor-premolar missing type, MSX1 plays a less important role in the development of this missing type. 46, 58 Moreover, PAX9 and TGFA have a role in the development of congenitally missing teeth by MSX1 and PAX9 interaction.49-52
The understood of the exact genetic mechanism responsible for the development of congenital teeth missing is still vague.20, 42, 51, 60 So independent mechanisms might recommend for each missing tooth.20 Nowadays, mutations in specific genes as LRP6 gene “gene encoding low-density lipoprotein receptor-related protein” has been reported for the etiology of the tooth absence.61
Materials and Methods
The study was undertaken on 395 patients (189 Males and 206 Females) aged ranged between 13 to 25 years who referred to some dentistry centers in Baghdad for taking “orthopantomogram” (O.P.Gs) for the period from December 2018 to November 2019.
All patients with O.P.Gs were examined clinically on the dental chair for diagnosis of the missing teeth and taking the history to confirm the congenital absence of teeth. The radiographs were viewed by an X-ray viewer.
A tooth was registered as a congenitally missing tooth when there was no evidence of any calcification in the missing tooth region on O.P.G radiograph, as well as when the missing tooth region is not due to tooth extraction or exfoliation. Figure 1 & 2.
All patients were informed of the purpose of the study with signed consents.
Exclusion criteria

Figure 1. A panoramic radiograph (O.P.G) showed bilateral congenitally missing upper lateral incisors.
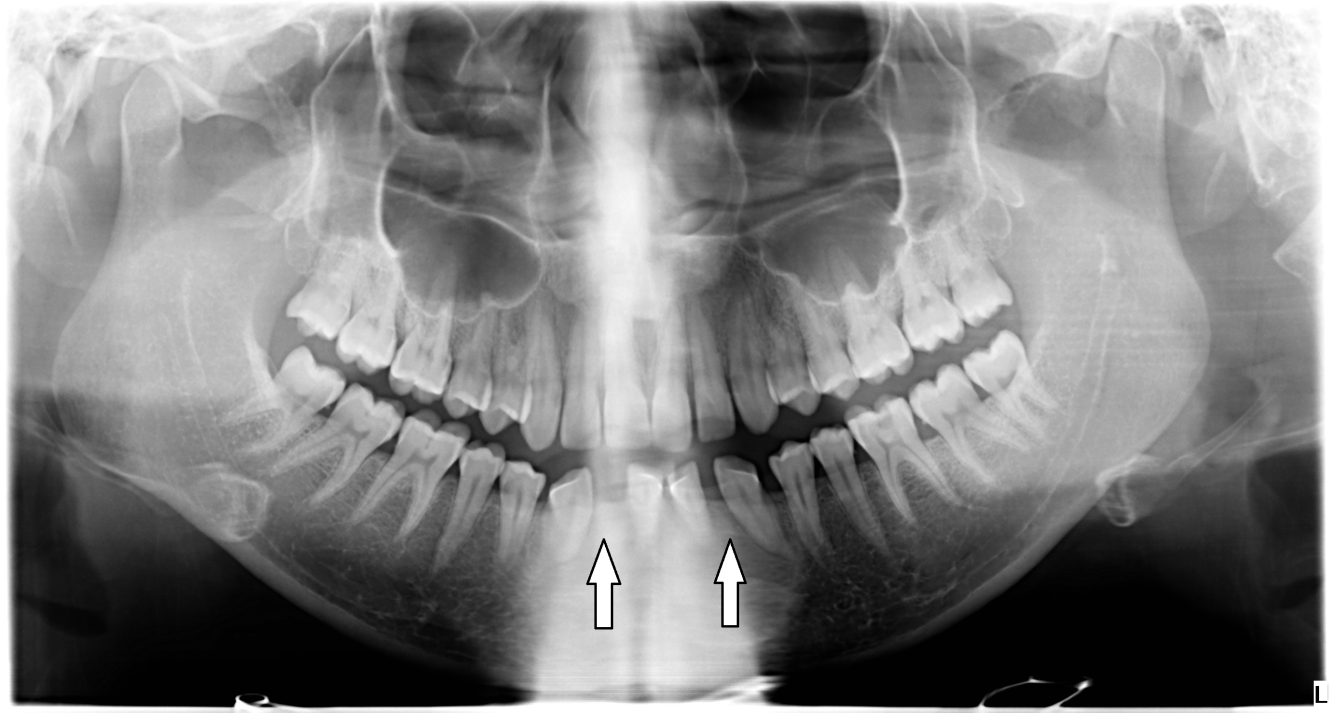
Figure 2. A Panoramic radiograph (O.P.G) showed bilateral congenitally missing lower lateral incisors.
Statistical Analysis
All data were analyzed using the Statistical Package for the Social Sciences software (version 19). The relation between the prevalence of CMT and gender, upper and lower jaws were analyzed using Pearson’s chi-squared test. The significance level was set at 0.05 and considered significant if the P-value < 0.05.
Results
The statistical analysis showed that most congenitally missing teeth in the current study were the maxillary lateral incisors in the percentage of 4.81%, followed by the mandibular second premolars (4.30%), mandibular lateral incisors (0.50%), maxillary central incisors (0.50%), and maxillary second premolars (0.25%) respectively. [Table 1] The study showed no any type of teeth agenesis for the other teeth. The results showed no significant increase in the prevalence of congenitally missing teeth in females (in the percentage of 11.16%) in comparison with males (9.52%). [Table 2] The results also showed no significant increase in the prevalence of congenitally missing teeth in the upper jaws (in the percentage of 5.56%) in comparison with lower jaws (4.81%). [Table 3] The study also showed no significant increase in the prevalence of unilateral congenital missing teeth (in the percentage of 3.16%) in comparison with the bilateral congenitally missing teeth (2.02%). [Table 4] Also, the study showed no significant increase in the prevalence of congenitally missing teeth on the left side of the jaws (in the percentage of 5.56%) in comparison with the right side (4.81%). [Table 5] According to these results, the rate of congenitally missing teeth in the current study was 10.37% of the study sample.
Table 1. Distribution of CMT in the maxilla and mandible.
|
Congenitally missing teeth (CMT) |
Maxillary arch |
Mandibular arch |
||||
|
Males |
Females |
Total |
Males |
Females |
Total |
|
|
Right central incisor |
0 |
1 |
1 |
0 |
0 |
0 |
|
Right lateral incisor |
4 |
3 |
7 |
0 |
1 |
1 |
|
Right canine |
0 |
0 |
0 |
0 |
0 |
0 |
|
Right first premolar |
0 |
0 |
0 |
0 |
0 |
0 |
|
Right second premolar |
0 |
1 |
1 |
5 |
4 |
9 |
|
Right first molar |
0 |
0 |
0 |
0 |
0 |
0 |
|
Right second molar |
0 |
0 |
0 |
0 |
0 |
0 |
|
Left central incisor |
0 |
1 |
1 |
0 |
0 |
0 |
|
Left lateral incisor |
4 |
6 |
12 |
0 |
1 |
1 |
|
Left canine |
0 |
0 |
0 |
0 |
0 |
0 |
|
Left first premolar |
0 |
0 |
0 |
0 |
0 |
0 |
|
Left second premolar |
0 |
0 |
0 |
3 |
5 |
8 |
|
Left first molar |
0 |
0 |
0 |
0 |
0 |
0 |
|
Left second molar |
0 |
0 |
0 |
0 |
0 |
0 |
Table 2. showed the frequency of CMT in males and females
|
Gender |
Number of CMT |
Percentage of CMT |
Chi-square test |
Significance level at 0.05 |
|
Males |
18 |
9.52% |
1.24 |
The p-value is 0.2 Not significant at p-value < 0.05 |
|
Females |
23 |
11.16% |
|
|
CMT: Congenitally missing teeth
Table 3. showed the frequency of CMT in maxilla and mandible
|
Type of jaw |
Number of CMT |
Percentage of CMT |
Chi-square test |
Significance level at 0.05 |
|
Maxillary jaw |
22 |
5.56% |
0.23 |
The p-value is 0.6 Not significant at p-value < 0.05 |
|
Mandibular jaw |
19 |
4.81% |
|
|
CMT: Congenitally missing teeth
Table 4. showed the frequency of unilateral and bilateral CMT in the jaws
|
CMT in both jaws |
Number of CMT |
Percentage of CMT |
Chi-square test |
Significance level at 0.05 |
|
Unilateral CMT |
25 |
3.16% |
2.08 |
The p-value is 0.1 Not significant at p-value < 0.05 |
|
Bilateral CMT |
16 |
2.02% |
|
|
CMT: Congenitally missing teeth
Table 5. showed the frequency of CMT in the left and right side of the jaws.
|
Side of jaw |
Number of CMT |
Percentage of CMT |
Chi-square test |
Significance level at 0.05 |
|
Left side |
22 |
5.56% |
0.23 |
The p-value is 0.6 Not significant at p-value < 0.05 |
|
Right side |
19 |
4.81% |
|
|
CMT: Congenitally missing teeth
Discussion
A congenitally missing tooth or tooth agenesis is considered to be one of the most anomalies in jaws compared to other dental anomalies that are distributed widely among the people of the world.
Many authors indicated that several factors could have a role in the incidence of dental anomalies, these factors varied as hereditary, environmental, the pattern of nutrition, chewing function and systemic problems.62-67
Several studies observed the prevalence of congenitally missing teeth all over the world. Graber stated that the ratio of congenitally missing teeth excepting the third molars were 1.6-9.6% in several studies in many countries.41 Other studies stated that the ratio was 2-16.3%.68-70 Also, the ratios in German and Malaysian populations were 12.6% and 2.8% respectively.49, 60 Sheikhi reported that the prevalence of congenitally missing teeth in the Iranian population was 10.9%.57
It was reported that the “teeth agenesis” occurred with the permanent teeth about two to nine times more than the deciduous teeth.18, 58
The prevalence of congenitally missing teeth found with high variation and distribution relative to gender, ethnicity, and race.26, 58, 69, 71-73 For example, Edward and Larkin studied the racial prevalence of congenitally missing teeth in black and white American people and the found that the prevalence was significantly more in white people compared to the black people.74
Other studies reported that environmental and genetic circumstances have an important role in the occurrence of the congenitally missing teeth. 41, 75
The current study observed the prevalence of congenitally missing teeth in a sample of the Iraqi population and also the correlation of the congenitally missing teeth prevalence between genders, upper and lower jaws, and as well as between the right and left side of the same jaw.
The results of current studies showed that most congenitally missing teeth in the current study were the maxillary lateral incisors, followed by the mandibular second premolars, mandibular lateral incisors, maxillary central incisors, and then maxillary second premolars. The study showed no type of “teeth agenesis” for the other teeth.
Many studies have agreed that maxillary lateral incisors are the most congenitally missing teeth followed by the mandibular second premolars.18, 60, 76-79
In many people also it has been reported that the most frequent congenitally missing teeth were the maxillary lateral incisors and then mandibular and maxillary second premolars respectively (except third molars).18, 60, 76, 77
The maxillary lateral incisor also reported being the most common congenitally missing tooth in some studies.20, 36 Also, the maxillary lateral incisor was reported to be the most prevalent congenitally missing tooth in several studies in Iranian12, Turkish,16 Brazilian,15 Sudanese,80 and Malaysian population.60
But on the other hand, some authors reported that the most prevalent congenitally absent teeth were, the mandibular lateral incisors,71 the mandibular central and lateral incisors.26 In another study in the orthodontic Iranian population, the most frequent congenitally missing teeth were the mandibular second and then the maxillary second premolars.57
Several studies also showed that the mandibular second premolars are the most congenitally missing teeth followed by the maxillary lateral incisors and maxillary second premolars.81-84
In some studies also it was reported that the mandibular second premolars were the most frequent congenitally missing teeth and then the maxillary lateral incisors and the mandibular central incisors respectively.17, 85
Also, other studies show that the mandibular second premolars are the most frequent congenitally missing teeth. The maxillary second premolar are second and then the maxillary lateral incisor and the mandibular central incisor respectively.21, 24, 25, 71, 86
In Europe, it was reported that the most common congenitally missing teeth are the mandibular second premolar following the third molar, and then the maxillary lateral incisor and maxillary second premolar.87
The study also found that congenitally missing teeth were more prevalent in females compared with males, this agreed with several studies.17, 18, 26, 80, 84, 88-91 Many studies had confirmed that the difference is not significant, but other studies have been stated that there was a high prevalence increase in females in comparison to males.14, 19, 20
But on the other hand, some authors in the Kenyan population reported that the most prevalent of congenitally missing teeth were in males rather than females.21
Also, the study found that the prevalence of congenitally missing teeth was more in the maxilla than the mandible but this difference was no significant. These findings are similar to many studies.15-17, 84, 92-94 But on the other hand, other studies stated that the majority of these absences were in the mandibular jaw.95-97
The study also showed that the prevalence of congenitally missing teeth on the left side of the jaws is more in comparison to the right side but this difference was not significant.
The study showed that the congenital absence teeth on the left side of the jaws were more prevalent compared with the right side but this difference was not significant. This agreed with the study of some authors and they found that the prevalence of congenitally missing teeth was more predominant (55%) on the left side in comparison to the right side of jaws which was 45%.98
Hazim found that the occurrence of the congenitally missing teeth was more prevalent on the right side compared to the left side of the jaws.94 Also, other studies found that the congenitally missing teeth were symmetrically distributed between the left and right side of jaws.16, 71, 77, 99
The current study also showed no significant increase in the prevalence of unilateral congenital missing teeth (61.29%) in comparison with the bilateral congenitally missing teeth (38.70%). But many authors found that the frequency of unilateral and bilateral congenitally absent teeth was similar.84
Overall, The current study found that the rate of congenitally missing teeth in the sample of the Iraqi population was 10.37%. The size of the study sample, genetic, and the local region where the study was conducted might affect the results.
Conclusion
The rate of congenitally missing teeth in the sample of the Iraqi population was 10.37%. The most prevalent congenitally missing teeth were the mandibular second premolars and the maxillary lateral incisors respectively.
Acknowledgement
My gratitude is to all dentistry centers where the study was done.
Financial support and sponsorship
Nil.
Conflicts of interest
There was no conflicts of interest.
References
Corresponding Author
Hussein Haleem Jasim
Department of Oral Diagnosis, College of Dentistry, University of Wasit, Kut city, Iraq
E-mail: hhaleem @ uowasit.edu.iq







