MARGINAL SEALING ABILITY OF BULK-FILL VS CONVENTIONAL COMPOSITES; A SYSTEMATIC REVIEW
Aljazi Mohammed Alajmi1*, Raghad Saeed AlAmoudi1, Reem Abdullah Ibn Juma1, Nouf Awadh Alotaibi1, Khalid Naif Alharbi2
1Department of Internship Training Program, College of Dentistry, Riyadh Elm University, Riyadh, KSA. [email protected]
2Department of General Dentistry, Thadiq Hospital, Ministry of Health, Riyadh, KSA.
https://doi.org/10.51847/N0ISckMEt9
ABSTRACT
Resin composites were first used as aesthetically pleasing materials for front dental restorations, and their use for posterior teeth followed swiftly. Composite restorations still have several shortcomings, even with the advancement of adhesive techniques and the development of composite resins. One of the main problems is polymerization shrinkage, which may cause debonding between the resin composite and tooth structure. This results in minor discoloration and secondary caries that might shorten the restoration's lifespan. Polymerization stress is also generated as a result of this phenomenon. Results indicated no significant differences in marginal microleakage among certain materials and application techniques. Bulk-fill composites demonstrated advantages in marginal adaptation, while the impact of different cavity configurations and storage times was noted. Some studies focused on specific types of cavities or utilized different storage conditions, making direct comparisons challenging. Future research should consider standardized protocols to enhance comparability. Moreover, investigating long-term performance, clinical outcomes, and patient satisfaction would provide a comprehensive understanding of restorative materials.
Key words: Sealing ability, Bulk-fill, Conventional composites, Randomized control trials.
Introduction
Resin composites were first used as aesthetically pleasing materials for front dental restorations, and their use for posterior teeth followed swiftly. Composite restorations still have several shortcomings, even with the advancement of adhesive techniques and the development of composite resins. One of the main problems is polymerization shrinkage, which may cause debonding between the resin composite and tooth structure. This results in minor discoloration and secondary caries that might shorten the restoration's lifespan. Polymerization stress is also generated as a result of this phenomenon [1].
Additionally, these forces can produce cusp displacement and microfractures by transferring into the tooth structure. The chemical formulation of some materials is one of the many attempts that have been undertaken to minimize the volumetric shrinkage of composite resins [2]. One of the most common issues with resin composites is microleakage. A marginal gap may form at the tooth restoration interface when there is a lack of sealing. Microleakage may develop at the tooth restoration interface if the stresses resulting from polymerization surpass the bond strength. These stresses are produced inside the restoration and at its borders [3].
The volumetric polymerization shrinkage, the resin composite's elastic modulus and flow, its adhesion to the cavity walls, and the restoration's configuration factor are some of the factors that affect the creation of stress. The ratio of the bonded cavities to the unbonded surface area is known as the cavity configuration factor or C-factor. A rise in the C-factor is linked to a gradual deterioration of the bond strength. As a result, the strength of the adhesive's interaction with the tooth structure should balance the polymerization stresses generated in the resin composite and at the interface. In the absence of this, gap development and marginal integrity may suffer. The viscoelastic characteristics of the material have a significant influence on the contraction stresses. These pressures could be transmitted to the restoration's margins in a clinical setting, lowering marginal quality. Problems including leaking, recurring cavities, and pulpal irritation might arise when marginal quality is insufficient [4].
Incremental filling procedures are often chosen over bulk filling methods to provide a successful marginal seal and prevent the clinical effects of polymerization shrinkage. Although the progressive method may be necessary for adequate light penetration, there are downsides, including the possibility of trapping voids within layers and the amount of time required to install the repair. Because fewer clinical stages are involved, the bulk application approach is easier to use and expedites the process. Thirteen Significant advancements in composite technology are rare, despite advancements in adhesive methods [5].
A line of goods known as "bulk fill composites" has just been released within this framework. Because of their strong responsiveness to light curing and decreased polymerization stress, these materials may be inserted in a 4 mm bulk placement. It ought to be coated with a traditional composite layer, subject to the material being used [5]. The current study aims to ascertain how much modern bulk-fill composites have changed from traditional composites in marginal adaption in various cavity designs. The assumption that there wouldn't be any variations in marginal adaption in cavities repaired using various composite materials was the null hypothesis analyzed.
Materials and Methods
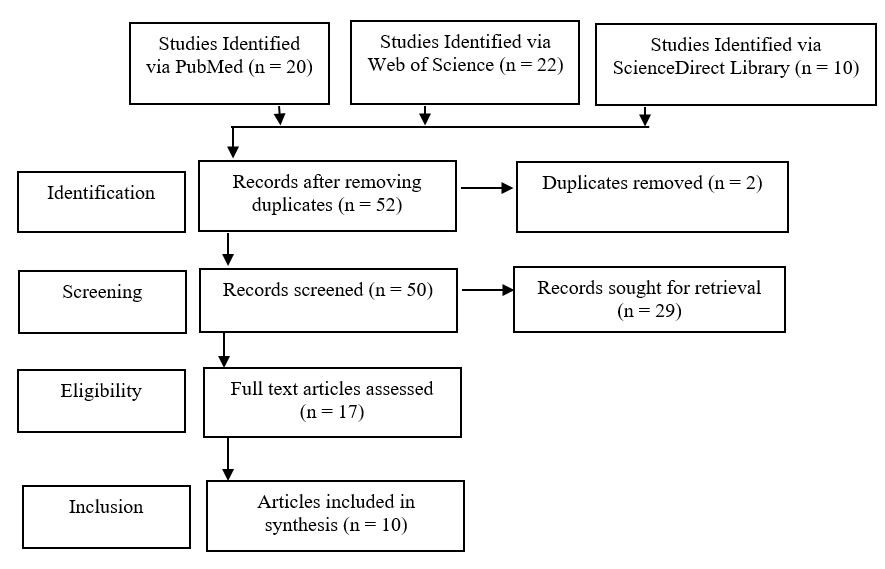
Using the PubMed, ScienceDirect, and Medline, databases, a comprehensive evaluation of the literature spanning 2010 to 2023 was conducted. The terms that were utilized were " sealing ability, bulk-fill, conventional composites, and Randomized control trials." To illustrate the procedure for choosing the articles to be searched for, a PRISMA schematic was employed (Figure 1).
Inclusion criteria
Exclusion criteria
|
|
|
Figure 1. PRISMA Flow Diagram |
Assessment of the risk of bias
The quality of the studies was evaluated using the Cochrane risk of bias assessment technique (Table 1).
Table 1. Summary of Cochrane Risk of Bias Assessment
|
Study |
Selection Bias/Appropriate control selection/baseline characteristics similarity |
Selection bias in randomization |
Selection bias in allocation concealment |
Performance-related bias in blinding |
Reporting bias/Selective reporting of outcomes |
Detection bias Blinding outcome assessors |
Accounting for confounding bias |
|
Shadman et al. [3] |
+ |
+ |
+ |
+ |
- |
+ |
+ |
|
Mohamed HI et al. [6] |
+ |
- |
+ |
+ |
+ |
+ |
+ |
|
Mosharrafian et al. [7] |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
GARCÍA et al. [8] |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
Aljamhan et al. [9] |
+ |
- |
+ |
+ |
+ |
+ |
+ |
|
Tavangar et al. [10] |
+ |
+ |
+ |
+ |
+ |
+ |
- |
|
de Albuquerque et al. [11] |
+ |
- |
+ |
+ |
+ |
+ |
- |
|
Abdelrahman [12] |
+ |
+ |
- |
+ |
+ |
+ |
+ |
|
Assiri et al. [13] |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
Yantcheva et al. [14] |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
Results and Discussion
Table 2 shows the summary of the included eleven studies, where the objectives, materials and findings have been listed. In class II cavities in maxillary premolars, Shadman et al.'s study [3] sought to evaluate and contrast the marginal dentinal microleakage of bulk fill (in two viscosities) and conventional composites. For this in vitro study, forty-two class II cavities extending 1 mm below the cementoenamel junction were made on both the distal and mesial surfaces of 21 maxillary premolars. Grandio composite was used to reconstruct the cavities in 2-mm increments, in contrast, 4-mm increments of X-tra fil and X-tra base were employed. After a 24-hour storage period at 37 °C and 100% humidity, they were sectioned, thermocycled (500 cycles, 5–55oC), maintained in basic fuchsine, and inspected under a stereomicroscope (×40). Between the groups, there were no significantly different variations (P=0.47) regarding marginal microleakage. In this regard, there was no discernible statistically significant change between the bulk and gradual application approaches (P=0.23).
The study's objective is to compare the marginal adaption of Sonic fill to Ceram X traditional composite resin composites, considering the impact of varying cavity configurations (C-factor). Ninety newly removed non-caries human premolar teeth were utilized, and they were randomly split into two equal significant groups (45 each) based on the tested materials: Sonicfill and Ceram X resin composites. Each group was then subdivided into three equal subgroups of fifteen based on the cavity configuration: class II cavities, class V cavities, and flat tooth surfaces. Each subgroup was subdivided into three five-month storage time intervals: one, three, and six months. The study's findings showed that Sonic-fill had less microleakage than Ceram X. Microleakage is not eliminated by C-factors for both bulk-fill resin materials. The smooth tooth surface in both class II and class V differed significantly. At six months of storage, Sonicfill and Ceram X had significant leakage scores Mohamed et al. [6].
The goal of the study conducted by Mosharrafian et al. [7] was to examine and contrast the microleakage of two bulk fills and one standard composite in class II restorations of primary posterior teeth. Sixty primary mandibular teeth that were second molars were used in this in vitro experiment and were split into three groups at random. Teeth with typical class II cavities were prepared, and the restorations used in groups 1 and 2 were Z250 conventional composite, SonicFill bulk fill composite, and 3M bulk fill composite. The mean (± standard deviation) dye depth of penetration in the gingival margins for 3M bulk fill, SonicFill, and Z250 conventional composite were 543±523μm, 343±290μm, and 597±590μm, in that order. In the occlusal margins, these values were 214±93μm, 302±127μm, and 199±145μm, in that order. Occlusal and gingival microleakage did not vary substantially among the three groups (P>0.05); however, in all three groups, gingival margins exhibited considerably more microleakage than occlusal margins (P<0.05).
The present experiment carried out by GARCÍA et al. [8] examined marginal microleakages of Class II cavities that were repaired using FiltekTM Bulk Fill, a bulk-fill resin, vs FiltekTM Supreme XTE, a traditional composite resin. Forty removed human teeth had two standardized Class II cavities made in them. For twenty molars (groups 1 and 2), the gingival border was positioned above the cementoenamel junction; for the other twenty (groups 3 and 4) (n = 20), it was positioned apically. When comparing the dentin margins to the gingival margins seen in enamel, there was a significant decrease in microleakage (p<0.01). There was no apparent distinction among either groups 1 and 2 (p=0.86) or 3 and 4 (p=0.26). Gingival microleakage in bulk-fill resins is comparable to that in traditional composites.
The current research done by Aljamhan et al. [9] set out to evaluate the effectiveness of various dental RBCs and techniques for class II cavity sealing of the deep dentin edge. Box cavities (class-II) were made on the distal and mesial surfaces of extracted premolar teeth, with the gingival margin 1 mm apical to the cementoenamel junction. Teeth with prepared class II cavities were randomly assigned to four study groups depending on the kind of restorative materials used (conventional RBC lined with flowable RBC, bulk-fill RBC, conventional RBC lined with resin-modified glass-ionomer-cement (GIC) as open sandwich technique, and conventional RBC). Each group was then separated into two subgroups: one called self-etch, which employed a self-etch adhesive method, and the other called total-etch, which used a separate etching phase before applying the bonding agent (n = 10). Group 4 (GIC) had the lowest dye penetration values, while group 2b—bulk-fill employing the self-etch adhesive system—followed with the highest values. The group Bulk-fill using the total-etch adhesive system (2a) reported the maximum dye penetration, followed by the group Conventional RBC using the total-etch adhesive system. Compared to the self-etch adhesive system (1a), the total-etch adhesive system exhibited much higher micro-leakage (p = 0.026).
The purpose of the Tavangar et al. [10] study was to compare microleakage in Class II cavities between bulk-fill composites (flowable, packable) and conventional light-cured composites. Sixty human removed premolars were used in this in vitro experimental investigation. We created typical Class II cavities in the teeth, measuring 1.5 mm in axial depth, 4 mm in height, and 3 mm in buccolingual length. Based on the kind of composite, the teeth were randomly divided into three groups: packable bulk-fill (x-tra fill packable; VOCO Company), flowable bulk-fill (x-tra base; VOCO Company), and conventional composite (Grandio; VOCO Company) comprised group I. According to the data, the bulk-fill packable and conventional composites' enamel and dentinal margins did not differ statistically substantially. (P= 0.06). Dentinal margins demonstrated more dye penetration to the axial surface's enamel edge in the bulk-fill flowable group (P<0.05). P<0.05 showed that there was no discernible variation in the marginal microleakage of enamel and dentin between the three groups.
de Albuquerque et al. [11] study's goal was to compare the volumetric shrinkage of bulk-fill vs standard composite resin, as well as the Class II mesial-occlusal-distal (MOD) restorations' marginal adaptation both before and after thermomechanical loading. A total of twenty-four human molars that were removed, undamaged, noncarious, and not repaired and kept in a 0.1% thymol solution were chosen. To fill in the teeth, the following was done: Group C: progressively filled with Esthet-X HD; Group B: bulk-fill with SureFil SDR flow as a basis (first increment, 4 mm) and covered with the conventional nanohybrid composite Esthet-X HD (second increment, 2 mm). Cluster A: utilize SureFil SDR flow for bulk filling (first increment: 4 mm; second increment: 2 mm). After light curing, the evaluated composites were put into a semi-spherical mold and placed within an AccuVol device to assess volumetric polymerization shrinkage. Groups A and B showed better marginal adaptation in the cervical dentin than Group C, both before and after loading (p< 0.05). Group B outperformed Group C in marginal adaptation to cervical enamel, whereas Group A's findings fell somewhere in between. Moreover, shrinkage was higher with bulk-fill flow than with Esthet-X HD.
The research conducted by Abdelrahman [12] sought to assess the bulk-fill flowable composite resins' shear bond strength and microleakage using self-adhesive resins. For this investigation, forty removed human teeth that were not carious were chosen. For the microleakage test, twenty Class V cavities were built on the labial surface. Ten teeth were treated: Group II was given a bulk fill flowable composite treatment together with a one-step self-etch adhesive system, whereas Group I was given a self-adhesive flowable composite treatment.he universal testing equipment was used to assess the shear bond strength. In both of the restorative materials under investigation, the mean microleakage score of the cervical margins was non-significantly greater than that of the occlusal margins. Compared to Vertise flow, Filtek flowable bulk fill composite showed a significantly higher mean microleakage score at the cervical and occlusal margins.
The purpose of the research done by Assiri et al. [13] was to assess and contrast the marginal adaptation of multilayer Filtek Z250 resin composite restorations, SonicFill bulk-fill resin composite, and class II (MOD) bulk-fill Tetric EvoCeram restorations. Thirty MOD cavities were made in human molar teeth that were removed. The cavities were separated into ten groups using three different restorative materials (Filtek Z250, Tetric Evoceram Bulk fill, and Sonic fill). A scanning electron microscope was used to evaluate marginal adaption. Comparing the typical bulk fill restorative material (Filtek Z250) with the investigated bulk fill materials (Tetric Evoceram Bulk fill and Sonic Fill), there were no significant differences (P<0.05).
In this investigation, fifteen human third molars that had been removed whole were employed. Based on the composites used, cavities were randomly split into three groups: Filtek Silorane LS-silorane, Filtek Ultimate-nanocomposite, and SonicFill-bulk-fill composite. After that, all specimens underwent heat cycles and were submerged in saline for ten mounds. Samples were aged and then submerged in 2% methylene blue. Once ready, they were immediately coated in gold and subjected to a SEM analysis to determine the marginal seal. Marginal fissures are much more prevalent now (p = 0.001). The microleakage research revealed a substantial influence of both substance (p < 0.000) and time (p < 0.000) [14].
Table 2. Key findings of included studies
|
Author's name |
Objective |
Sample Size |
Restorative Materials |
Main Findings |
|
Shadman et al. [3] |
Evaluate dentinal marginal microleakage |
42 maxillary premolars |
Grandio composite, X-tra fil, X-tra base |
No significant differences among groups in marginal microleakage; no difference between bulk and incremental application |
|
Mohamed HI et al. [6] |
Evaluate the C-factor effect on marginal adaptation |
90 premolars |
Sonicfill, Ceram X |
Sonicfill showed less microleakage; C-factors didn't eliminate microleakage; the significant difference between flat tooth surface and class II/class V |
|
Mosharrafian et al. [7] |
Compare microleakage of bulk fill and conventional composites |
60 primary molars |
3M bulk fill, SonicFill, Z250 conventional composite |
No significant differences in occlusal or gingival microleakage among the groups |
|
GARCÍA et al. [8] |
Compare microleakage of bulk-fill and conventional composites |
40 extracted molars |
Filtek Bulk Fill, Filtek Supreme XTE |
Lower microleakage in enamel vs. dentin margins; no significant difference between bulk-fill and conventional composites |
|
Aljamhan et al. [9] |
Assess dental restorative materials for sealing deep dentin |
Class-II cavities |
Conventional RBC, Bulk-fill RBC, GIC |
GIC showed the least dye penetration; total-etch had greater micro-leakage than self-etch |
|
Tavangar et al. [10] |
Compare microleakage between bulk-fill and conventional composites |
60 premolars |
Bulk-fill packable, Bulk-fill flowable, Conventional composite |
There is no significant difference in marginal microleakage among the three groups |
|
de Albuquerque et al. [11] |
Evaluate marginal adaptation before and after loading |
24 molars |
SureFil SDR flow, Esthet-X HD |
Bulk-fill had superior marginal adaptation in cervical dentin; bulk-fill flow resulted in more significant shrinkage. |
|
Abdelrahman [12] |
Compare microleakage and shear bond strength |
40 molars |
Self-adhesive flowable, Bulk-fill flowable |
Filtek flowable bulk fill showed higher microleakage; no significant difference in shear bond strength. |
|
Assiri et al. [13] |
Compare marginal adaptation of bulk-fill and conventional composites |
30 molar cavities |
Tetric EvoCeram, SonicFill, Filtek Z250 |
There are no significant differences in marginal adaptation among tested materials. |
|
Yantcheva et al. [14] |
Assess microleakage after thermal cycles. |
Fifteen extracted intact human third molars. |
Filtek Ultimate, Filtek Silorane LS, SonicFill |
Significant increase in marginal fissures; impact of time and material on microleakage |
In the early 2000s, there was a proposal to create a composite resin that was more translucent than earlier composites and appropriate for thicknesses up to 2 mm. Cusp flexure, gap formation, and shrinkage stress during polymerization may be decreased by altering the monomer composition, and all without reducing the degree of conversion may be decreased by altering the monomer composition [15]. A dependable marginal seal is crucial for cavity repair as it averts microleakage and its associated medical complications.
The primary benefits of bulk fill composites are reduced polymerization shrinkage due to changes in the organic matrix's or filler's composition and improved curing depth because of increased transparency and more effective initiator systems [16]. It has been reported that in some bulk-fill composites, a gradual increase in the elastic modulus during curing is caused by delayed polymerization, which reduces stress without increasing the overall rate of composite conversion.
According to the study's findings, all resinous materials had somewhat greater marginal adsorption after a month of storage. The shorter time that has passed since the water was stored or the adhesive system's strength throughout this time may be the reason for the improved marginal adaption. A solid hybrid layer can withstand debonding and provide an excellent marginal seal. When a resin-based composite is exposed to water, it begins to absorb water; the quantity of water absorbed varies and becomes more extensive. Water sorption influences the link between dental tissue repair via plasticization, hydrolysis, and oxidation [4].
The study's findings support the null hypothesis as there was no discernible difference in microleakage between bulk fill and conventional composites at the dentinal edge (P=0.47). Additionally, there was no discernible difference between the two bulk-fill composite viscosities. Many publications have reported similar findings and found no difference between the incremental conventional filling approaches and the marginal adaption of bulk filling [17]. According to research by Alamassi et al. [18], flowable bulk-fill composites had a faster rate of gap formation than bulk-fill composites that are traditional and non-flowable. When employing a progressive application technique, bulk-fill composites produced cervical margins of higher quality than traditional composites in research conducted by Par et al. [19]. Our findings are consistent with the notion that flowable bulk fill composites with lower polymerization stress are more pliable before reaching the gel point [16]. The shrinkage value of the X-tra base is 2.7%, which is within an acceptable range [18]. Parra et al. [17] reported that in tooth-restoration interfacial debonding, bulk-fill composites with good consistency were equivalent to conventional incremental composites. Similar to the findings of our investigation, In class II composite restorations, Park et al. [20] reported no change in gap size between bulk filling (using bulk fill composites) and progressive application (using conventional composites).
Mohamed et al. [6] employed the same scoring system as our study to compare the microleakage of conventional composites in primary molar teeth between two kinds of bonding chemicals (Clearfil Mega Bond and Scotchbond Multi-Purpose). They reported scores of 0 and 1 in both groups. In almost 70% of the patients in our research, there was traditional composite leakage up to sixty-seven percent of the gingival floor. Our findings vary from theirs, which might be caused by the thermocycling methodology, different bonding agents, or different dyes (because they employed methylene blue). In bulk fill composites, leakage results were better because dye penetration depth was limited to the outside sixty-seven percent of the gingival floor in 85% to 90% of the cases.
Considering the materials employed in this investigation, the findings indicated that low C-factor (O) produced low leakage scores for both sonic fill and Ceram X. In contrast, high C-factors (F) demonstrated significant leakage scores for both sonic and bulk fill. The fact that the quantity of polymerization shrinkage affected the adaption at the resin-cavity contact supported this conclusion. The material's flow does not release stresses caused by this shrinkage. Conversely, a lower C-factor number (O) permitted greater relaxation of the resin composite, reducing the shrinkage stresses produced during the polymerization process and thus reducing leakage [21]. The C factor and placement methods have an impact on how shrinkage stresses are modified. The degree of stress is mediated by the composite's stiffness, capacity to release tension, velocity of curing, and the restriction placed on it by bonding to the cavity preparation [22]. Internal tensions will be kept to a minimum if composite polymerization proceeds unrestricted. Due to the expectation of a reduction in the C-factor, the bulk fill and gradual fill strategies have been mainly endorsed. According to a previous study comparing the mechanical properties of bulk-fill composites, Venus Bulk Fill has mechanical properties (flexural strength, flexural modulus, and Vickers hardness) that are either less than or comparable to those of all the other bulk-fill composites (Tetric EvoCeram Bulk Fill, Surefil SDR, and SonicFill) [23]. It has been proposed that shrinkage is less significant for evaluating stress than elastic modulus [24]. In this way, the behavior of restorative materials under stress is influenced by their elastic modulus.
It is likely that specific flowable composites with low elastic modulus partly absorb the composite shrinkage strain, which results in their effective stress reduction [4]. The contraction stress increases with the composite's elastic modulus and polymerization shrinkage. Although flowable composites' significant volumetric shrinkage may result in high stress levels. Additionally, it's possible that their low elastic modulus will reduce stress buildup and maintain marginal integrity. However, adequate stress relief cannot be guaranteed when flowable composites with an elasticity modulus of at least 5 GPa are employed [5]. based on established elements for preventing microleakage, such as therapeutic material molecular elasticity, solvent structure, bonding resistance, and wetting and application characteristics. The bond contract's strength and modulus of elasticity decrease in the presence of water. The hydrophilicity of its component monomers determines the water sorption capacity.
Conclusion
The studies collectively explored various aspects of dental restorative materials, focusing on microleakage, marginal adaptation, and shear bond strength. Results indicated no significant differences in marginal microleakage among certain materials and application techniques. Bulk-fill composites demonstrated advantages in marginal adaptation, while the impact of different cavity configurations and storage times was noted. Additionally, the studies highlighted the influence of adhesive systems on microleakage. Overall, these findings contribute valuable insights into the performance of different dental restorative materials in various clinical scenarios.
Study limitation
Studies include variations in sample sizes, methodologies, and specific restorative materials tested. Some studies focused on specific types of cavities or utilized different storage conditions, making direct comparisons challenging. Future research should consider standardized protocols to enhance comparability. Moreover, investigating long-term performance, clinical outcomes, and patient satisfaction would provide a comprehensive understanding of restorative materials.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: This study is exempted from ethical approval.