Vitamin D is one of the steroid hormones that is mainly obtained from food and diet supplements and exposure to sunlight. This vitamin plays a vital role in bone turnover and calcium phosphate homeostasis and as a result the musculoskeletal system. In addition, vitamin D is important in the immune system. This research aimed to review the manifestations of vitamin D deficiency in the mouth, jaw, and face. In this review study, articles published in the English language between 2010 and 2024 were searched in Scopus, Google Scholar, Medline, and PubMed databases. By examining and studying several articles about vitamin D's role in various structures of the body including the mouth and teeth, the impacts of its deficiency in the occurrence of the disease, and the utilization of its supplements in disease recovery, it concludes that this vitamin plays a prominent role in the mouth and teeth health and it has an immune system. Although there were conflicting findings about the impact of vitamin D on external root resorption in Sjogren's syndrome and orthodontics. Therefore, clinical trial research is necessary to confirm the hypotheses.
Introduction
Throughout a person's life, nutrition affects the health of the body, including the integrity and function of the teeth and supporting structures of the mouth. A balanced diet plays a key role in this regard. Malnutrition occurs if the diet does not provide the vitamins, minerals, and other nutrients needed to support body tissues. In addition, the administration of some drugs can also cause nutritional deficiencies [1, 2]. Vitamins are important organic Ingredients that act as catalysts for body metabolic reactions, transcription factors, antioxidants, and electron donors. To date, 13 vitamins have been identified, and for each of them, the minimum required amount has been determined to be sure of their nutritional deficiencies [3, 4].
Among these vitamins is vitamin D, which plays a vital role in restoring calcium phosphate homeostasis as a result of the system of musculoskeletal. Also, this vitamin is efficient in the body's immune system [5, 6].
Vitamin D deficiency has a high prevalence so almost 40% of people in Europe have vitamin D deficiency and 13% have a severe deficiency. Vitamin D can enter the body through food supplements or be synthesized in the skin under the ultraviolet rays influence, but due to environmental and individual characteristics, the amount of vitamin D made in the body is not enough [7].
Vitamin D with anti-inflammatory, anti-cancer, and anti-bacterial effects and regulation of calcium metabolism it plays a vital role in the health of oral tissues such as oral mucosa, bones, teeth, and periodontium [8, 9]. But until now, the impacts of vitamin D on oral cavity health have received little attention, and therefore this issue requires further investigation. The purpose of this review is to investigate the vitamin D role in the body, especially in dentistry, and the manifestations of its deficiency in the mouth and teeth.
Materials and Methods
In this review study, articles published in the English language between 2010 and 2024 were searched in Scopus, Google Scholar, Medline, and PubMed databases. In this study, the keywords "vitamin D deficiency", "oral manifestations", "teeth", "vitamin D", and "medical dentistry" were searched.
Studies with insufficient or irrelevant data were excluded from the review. The included studies met the inclusion criteria, including articles related to the vitamin D role in dentistry and oral diseases.
Results and Discussion
Structure of vitamin D and its receptor
Vitamin D is one of the steroid hormones that is mainly obtained from food and diet supplements and exposure to sunlight. The two main shapes of vitamin D are vitamin D3 and D2 or ergocalciferol. Vitamin D3 is formed in the skin after exposure to sunlight. But vitamin D2 is obtained from food. Biological activation of this vitamin may also occur in oral tissues. Vitamin D levels below 25 nmol/L are considered deficient. The most common systemic effects of its deficiency are osteomalacia in adults and rickets in children [5]. Risk factors of vitamin D deficiency include premature birth, female gender, genetics, old age, obesity, malabsorption, more skin pigmentation, and urbanization [10].
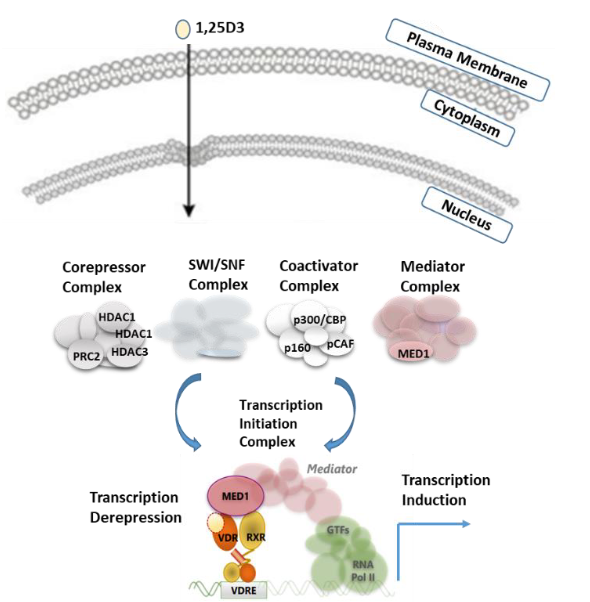
The mechanism of action of vitamin D is both extragenomic and genomic. Genomic action is mediated by the vitamin D receptor (VDR), which is related to the subfamily of nuclear receptors.
Figure 1 shows the schematic model for VDR (vitamin D receptor) regulation.
|
|
|
Figure 1. Schematic model for VDR (vitamin D receptor) regulation. |
Vitamin D receptors sustain skeletal structure and function and are found in bones, kidneys, parotid glands, skin, brain, and immune cells. Some specific alleles of the VDR gene affect the function of vitamin D at the cellular level. Anti-fibrosis and anti-inflammatory, Calcium metabolism, diabetic nephropathy prevention, proteinuria reduction, blood pressure, and atherosclerosis are among the functions of VDR [11]. The extra genomic effects of vitamin D are carried out by receptors with a different structure than the nuclear VDR, which includes the activation of cellular kinases and proteases and the release of the prostaglandins, which leads to the stimulation of some cells (monocytes, enterocytes, muscle, vascular smooth cells, chondrocytes, and osteoblasts) [12].
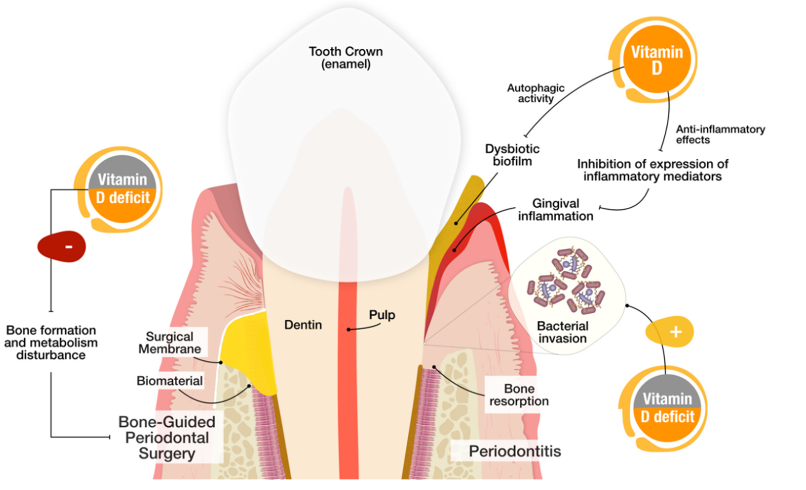
Vitamin D's role in dentistry and the effects of its deficiency in oral diseases are shown in a diagram in Figure 2.
|
|
|
Figure 2. Vitamin D's role in dentistry and the effects of its deficiency in oral diseases. |
Vitamin D in pediatric dentistry
Tooth decay
Vitamin D deficiency may be related to increased caries risk by affecting calcium metabolism and calcification of teeth during hard tissue formation [13]. This vitamin plays an important role in the formation of dentin, enamel, and bone because odontoblasts and ameloblasts are the vitamin D target cells. Its deficiency during the time of tooth formation may lead to developmental defects including enamel hypoplasia, which is an important risk factor for Severe Early Childhood Caries (ECC) which is at risk of caries. They are teeth. Deficiency of calcium and vitamin D, gestational diabetes, and neonatal hypoxia are causes of enamel defects in milk teeth [14]. Vitamin D levels before birth, childhood, and improvement of vitamin D status in pregnant women may affect the ECC rate of newborns [15, 16].
Tooth growth
Disruption of tooth growth is a common result in children. Nutritional deficiency, systemic disorders, hormone deficiency, and syndromes can also be related to a PPT (persistent primary tooth) and DTE (delayed tooth eruption). In a study, Brazilian children with PPT had lower vitamin D levels, and children with vitamin D deficiency were more exposed to DTE. Therefore, the significance of vitamin D concentration of mother and baby for the development of milk teeth is emphasized. Low levels of vitamin D in mid-pregnancy or at birth have been related to delayed eruption of milk teeth [17].
Vitamin D and orthodontics
In a study, it was found that clinical factors and polymorphism of vitamin D receptors are related to root apical external analysis in orthodontic patients. In Khalaf's study, the rate of tooth movement in orthodontics was not affected by vitamin D deficiency in rats [17]. In Azizi's study, the vitamin D serum level had no significant relationship with root external analysis [18]. Al-Attar's study stated that having an optimal level of vitamin D3 reduces alignment time and pain associated with orthodontic treatment [19]. Systemic administration of VitD reduced the rate of orthodontic tooth movement by creating more resistance in the bone but also contributed to less treatment relapse due to greater bone mineral density [20].
Vitamin D and periodontium
Vitamin D has several roles in preserving periodontal health. Its active form 1,25-(OH)2D3 is essential in the regulation of genes through the hydroxylase enzyme, which encodes proteins needed for adhesion and connections in epithelial cells, which strengthens and improves the physical barrier made by epithelial cells and improves cell-to-cell communication. Vitamin D is a potent inducer of antimicrobial peptides, involved in innate immunity, which may have neutralizing and antibacterial activity of lipopolysaccharide against periodontal pathogens [21].
Vitamin D can also induce the antimicrobial peptides production such as cathelicidin and some defensins, which protect the individual against oral pathogens. The antimicrobial impacts of vitamin D are mediated by VDR and are related to the cathelicidin hCAP-18 gene regulation [22]. It has been found that 1,25-(OH)2D3 can induce monocytes to differentiate into macrophages, which increases the activity of lysosomal enzymes and phagocytosis. In addition, this form in vitro synthesizes macrophage mRNA, inhibits IL-1, IL-6, and TNFa, and suppresses these proinflammatory cytokines synthesis. Vitamin D can increase the chemotactic and phagocytic capacity of macrophages. Vitamin D or calcium reduces alveolar bone loss and gingival inflammation. VDR gene polymorphisms are related to periodontitis, alveolar bone loss, or tooth loss. Taking vitamin D and calcium supplements may inhibit alveolar bone loss, increase bone mineral density in the mandible, and improve periodontal health. Periodontal patients in the maintenance phase who consume vitamin D and calcium supplements had better periodontal health compared to those who do not consume these supplements. Therefore, sufficient vitamin D can have a positive effect on the recovery rate of periodontal treatments. Radiographic examinations also showed these effects. 1α, 25-dihydroxyvitamin D3 (1,25-D 3) treatment increases osteogenic differentiation of human periodontal ligament stem cells [23].
Vitamin D in reconstructive and implant surgeries
Since dental implant osseointegration depends on the bone regeneration ability, it is thought that the process of healing and the bone tissue formation around the implant decreases with vitamin D deficiency. In some cases, premature failure of dental implants has been reported in patients with vitamin D deficiency [24].
The appropriate concentration of this vitamin is potentially related to the success of all stages of implant osseointegration, as it has a positive effect on regeneration metabolism as well as on continuous bone regeneration around the implant after loading. There was a significant relationship between the increase in serum vitamin D level and the osteoclast's presence around the graft particles during augmentation. The impact of vitamin D mixed with xenograft on alveolar bone augmentation and improved bone shape and implant stability was observed [25]. The peri-implant bone levels were higher in patients who took vitamin D supplements [26]. In Garg P's study, a significant relationship was observed between the marginal bone amount in vitamin D deficiency patients who received vitamin D supplementation and those who did not receive it [26].
Some studies stated that the impact of the level of vitamin D on implant osseointegration is controversial [27]. According to Alsulaimani's review, it is difficult to find a direct causal relationship between early dental implant failure and low serum vitamin D levels. The serum level of vitamin D may play a vital role in osseointegration and the success of dental implants or in predicting the survival rate of dental implants through its impacts on regulating the immune system and the healing process [28]. A systematic review showed that vitamin D serum levels in patients may play a role in the osseointegration of marginal bone loss and survival of dental implants. It is recommended that the serum vitamin D level of each patient be determined before dental implant placement and that vitamin D supplementation be provided if necessary, although more randomized human clinical trials are required to confirm this hypothesis [29]. Vitamin D can help reduce bacterial infections and peri-implantitis. A significant reduction in serum 25(OH)D was observed in the control group compared to the control [30].
Vitamin D and oral diseases
Bone and joint diseases
MRONJ (Medication-related osteonecrosis of the jaw) is a position in the oral cavity that leads to the disposal of the underlying necrotic bone. This is a severe late complication associated with the antiangiogenics and bisphosphonates denosumab, which are prescribed in the treatment of certain cancers and osteoporosis. Vitamin D can be effective in bone repair in patients with osteonecrosis caused by bisphosphonate. Since MRONJ can occur in all oral surgeries, it can be prevented by taking a history, consulting with a doctor, and using surgical or less damaging techniques such as lasers. Research has shown that not only vitamin D, but also PTH levels have a significant effect on the risk of osteonecrosis of the jaws, and also vitamin D deficiency can cause disturbances in PTH calcium levels [31]. Vitamin D supplementation may have a protective effect against diseases that later require the use of bisphosphonates, which can cause osteonecrosis of the jaw, and as a form of primary prevention against diseases in which the risk of ONJ increases [32].
Vitamin D and temporomandibular joint disorder
Several studies investigated the vitamin D effect on temporomandibular joint and daily activity and it was revealed that vitamin D deficiency is related to pain and affects the daily activity of patients [33, 34]. In Demir's study, vitamin D serum levels in temporomandibular joint disorder patients were not different compared to the healthy group. In addition, in patients with temporomandibular joint disorder, the level of parathyroid hormone increased due to vitamin D deficiency, therefore, in patients with temporomandibular joint disorder, vitamin D deficiency should be assessed and corrected [35, 36]. The results of a systematic review showed that the serum level of vitamin D was often lower in patients with temporomandibular joint disorder, and the evidence related to VDR polymorphism in these patients was noticed. Vitamin D serum levels and VDR may play a role in the onset and progression of temporomandibular joint disorder. However, the mechanisms of these relationships have not been fully determined, so more studies are needed [34].
Vitamin D and oral cancer
Studies emphasize vitamin D's importance in cancer prevention due to its cellular function (anti-apoptotic, anti-inflammatory, anti-angiogenic, anti-invasive, anti-metastatic, and anti-proliferative) on cancer cells. The active form of vitamin D applies its biological activities by binding to the nuclear VDR in various tissues. Because a wide range of tumor tissues express VDR, this receptor has the potential to influence cancer etiology [35].
Oral supplementation of this vitamin increased the efficacy of photodynamic therapy for the death of squamous cell carcinoma tumor cells in mice. Therefore, topical systemic vitamin D may be a new adjunctive non-toxic supplement for cancer treatment. The active form of this vitamin increased the expression of the VDR protein and gene in various types of cells in laboratory conditions. Yuan's study supported the role of vitamin D signaling in oral keratinocyte pathophysiology in vivo and in vitro. However, it seems that vitamin D deficiency alone is not enough to stimulate carcinogenesis and alter the homeostasis of the oral epithelium. Afzal showed that low plasma vitamin D levels were related to an increased risk of smoking-related cancers (squamous cell carcinoma of the head and round). All VDR gene polymorphisms are not equally associated with cancer, and the significance of each polymorphism is determined by the location of the cancer. It is also necessary to evaluate the relationship between VDR and other environmental factors of diet and lifestyle that are related to cancer [36]. Sundaram's study showed that vitamin D inhibited the growth of various OSCC tumor-derived cell lines [37]. Some processes related to this vitamin can regulate the expression of cytochrome 21 P450 and inhibit the proliferation of OSCC cells. Vitamin D analogs have potential therapeutic agents to control the progression of OSCC.
Vitamin D and oral mucosa diseases
The vitamin D serum level in Recurrent Aphthous Stomatitis was significantly lower than that of healthy subjects, but it is not clear whether vitamin D deficiency is the cause or consequence of this disease [35, 37]. Even though treatment or supplements have no significant side impacts, recommending vitamin D as an appropriate treatment option is controversial [36]. Nemati et al. [38] reported that vitamin D deficiency is a vital factor in the immunologic response in PFAPA syndrome, in which canker sores are associated with febrile episodes of pharyngitis and cervical lymphadenopathy. The level of vitamin D in these patients was significantly lower than in the control group.
There are conflicting results on the impacts of vitamin D levels on the growth and course of Sjogren's syndrome. Bang and Muller observed an inverse relationship between the serum level of this vitamin and the clinical symptoms severity and the inflammatory markers concentration in early Sjogren's syndrome. However, Baldini and Szodoray did not observe a decrease in vitamin serum levels in primary Sjogren's syndrome [39].
There is a strong association between vitamin D and oral candidiasis. With a lack of vitamin D, calprotectin increases in the blood, the function of neutrophils decreases, and the risk of opportunistic infections increases [40]. Vitamin D deficiency in AIDS patients increases the incidence of oral candidiasis. The number of CD lymphocytes is less than 200 and lack of vitamin D are environmental factors causing candidiasis in these patients [40].
Oral lichen planus (OLP) is a chronic mucosal skin disease that is observed with periods of exacerbation and remission. Because vitamin D has anti-inflammatory and immune system regulatory properties along with a regulatory effect on the proliferation and differentiation of keratinocytes, its possible role in the treatment of OLP was considered. In a systematic review, all included studies demonstrated a significant improvement in OLP symptoms in patients who received vitamin D supplementation as adjunctive therapy to conventional steroid therapy or placebo. Further studies with larger sample sizes are needed [41].
Vitamin D and the oral microbiome
Many oral diseases (caries and periodontal disease) are associated with homeostasis disorders. The host's immune system produces antimicrobial peptides (AMPS) that are effective in controlling the oral microbiome, maintaining health, and the occurrence of oral pathologies [42, 43]. Dental mesenchymal stem cells may play a role in antibacterial defense through the production of antimicrobial peptides by absorbing phagocytic immune cells and regulating their activity. These effects are increased by an inflammatory environment and are influenced by vitamin D.
Conclusion
The current study reviewed the vitamin D role in different departments of dentistry, and the results of the study showed the high importance of this vitamin in the health of the mouth and teeth. Since vitamin D deficiency is very common, it is very important to know the role of this vitamin and to provide a sufficient amount of it, and evidence shows that the biological activation of this vitamin may also occur in oral tissues [44].
The role of this vitamin in oral and dental health starts from the beginning of the fetal period so the low level of vitamin D in a pregnant mother is associated with increased caries and impaired growth of the baby's teeth. Vitamin D deficiency is more common in the second and third trimesters of pregnancy. Therefore, intervention programs to raise awareness about its importance during pregnancy should be considered. Another role of this vitamin is in the movement of teeth in orthodontic treatment, where studies have been associated with conflicting findings on the impact of vitamin D on the external analysis of the root [27, 29]. Vitamin D has a protective role against periodontal diseases through bone preservation and anti-inflammatory and antibacterial activity [31]. Other effects that vitamin D has on bones can help improve TMJ joint pain and bone repair caused by osteonecrosis, but more research is needed [45, 46].
Vitamin D deficiency has been seen in patients with oral cancers, but according to Yuan's study, it is not enough to cause cancer. Another controversial issue regarding vitamin D deficiency in Sjögren's syndrome is that the serum level of this vitamin is not a definitive factor in patients with this disease [47]. However, vitamin D deficiency has been seen in patients with oral candidiasis, but it does not affect denture stomatitis and is related to candidiasis. The impact of vitamin D on oral lichen planus has been successful [48]. If vitamin D levels are low due to systemic diseases such as rickets, kidney diseases, and IBD, it can have oral manifestations on bones and teeth. The prominent role of vitamin D, which is known today, is in increasing the body's immune system through the production of antibacterial peptides to deal with opportunistic viral or fungal infections. Lack of vitamin D in the body can also increase various respiratory tract infections, including Covid-19 [49].
According to the studies, vitamin D's role in oral and dental health is important as well as general health, and the lack of this vitamin has harmful effects, especially on oral and dental health. Therefore, written programs to supply this vitamin in the health system of the communities are recommended.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None