WOUND HEALING OF CYANOACRYLATE VS COLLAGEN AMONG PATIENTS UNDERGOING ORAL SURGERY; A SYSTEMATIC REVIEW
Shahzeb Hasan Ansari1*, Suhael Ahmed1, Linda Nabeel Abdulaziz2, Sara Mohammed AlRumayyan2, Menatallah Abdelwahab Mostafa2, Rahaf Sultan Al-Mohammed2, Sharifah Hussain AlFarhan2
1College of Dentistry, Riyadh Elm University, Riyadh, KSA. [email protected]
2Department of Internship Training Program, College of Dentistry, Riyadh Elm University, Riyadh, KSA.
https://doi.org/10.51847/kFJklR9Vtt
ABSTRACT
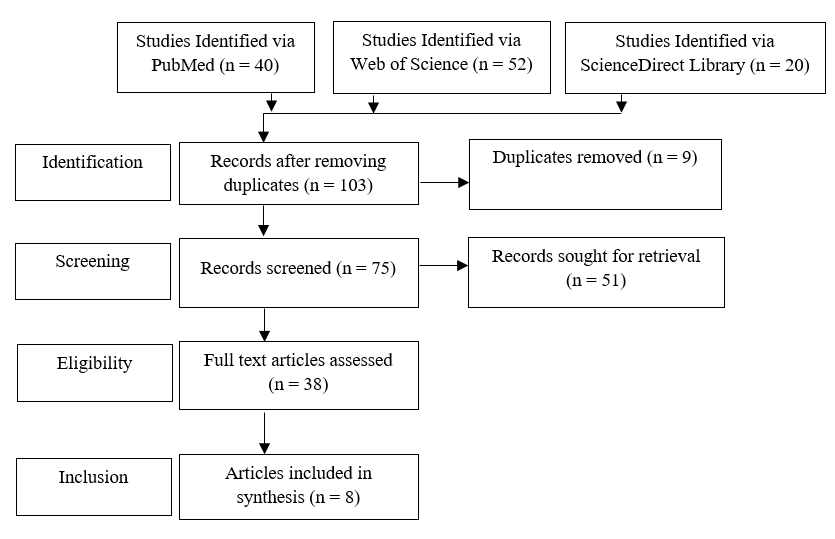
Intraoral wounds are susceptible to infection, and this has been quoted as one of the significant justifications for postoperative wound dehiscence and discomfort. An intraoral dressing that is moisture-proof and adherent, poses a perfect answer to safeguarding the surgical site. Such a dressing may shield the wound from physical, thermal, or bacterial harm as a result of consumption of food or contamination by saliva. The purpose of this systematic review is to compare cyanoacrylate and collagen when it comes to successful intra-oral wound healing. The systematic literature review was performed using articles from 2012 to 2023 in databases such as PubMed, Medline, and Science Direct. The PRISMA flowchart is used to describe the selection process of searched articles. A total of 8 articles were finalized and used in this systematic review. It was concluded that using cyanoacrylate tissue glue as a defense mechanism instead of an exposed collagen barrier membrane was superior. They are effective for site management and hemostasis because they have both bacteriostatic and hemostatic qualities. Cyanoacrylates were discovered to have less inflammation as compared to collagen wound dressing material.
Key words: Cyanoacrylate, Collagen, Wound dressing, Randomized control trial.
Introduction
Intraoral wounds are susceptible to infection, and this has been quoted as one of the significant justifications for postoperative wound dehiscence and discomfort. An intraoral dressing that is moisture-proof and adherent, poses a perfect answer to safeguarding the surgical site. Such a dressing may shield the wound from physical, thermal, or bacterial harm as a result of consumption of food or contamination by saliva [1].
Collagen dressing has widely been consumed in dentistry because of its capacity to accomplish hemostasis, being chemotactic to fibroblasts and platelets, and encouraging mesenchymal proliferation and separation [2]. CollaCote ® is an extremely porous absorbable type I Bovine Collagen wound dressing invented from bovine deep flexor tendon. It regulates bleeding and steadies blood clots in addition to shielding the wound site while speeding up the healing process [3].
Resorbable collagen membranes (RCMs) are constructed from allogeneic or xenogeneic foundations to cope with the oral wounds for instance extraction sockets, for periodontal or endodontic surgeries. They play their part as platforms for bone deposition in guided bone regeneration (GBR), stimulate platelet accumulation, stabilize clots, and invite fibroblasts, expediting wound healing [4]. They are intended to resorb in 2 to 32 weeks and are biocompatible, convenient to handle, and only slightly immunogenic. They exist in the form of membranes, plugs, or pads for comfort of utilization. Even though resorbable collagen membrane is aimed to be quite readily resorbable, this substance occasionally continues to stay within wound sites devoid of any apparent foreign body reaction [5].
N-butyl cyanoacrylate (PeriAcryl 90) is among the biocompatible tissue adhesion materials that exhibit anti-bacterial and hemostatic outcomes. PeriAcryl®90 is a cyanoacrylate tissue adhesive that has become a widespread product in oral surgery. This dental adhesive is intended to perform precisely in the oral cavity. PeriAcryl®90 is a perfect mixture of n-butyl cyanoacrylate and 2-octyl cyanoacrylate that provide the formulation with the ideal set of features to function on soft oral tissue. PeriAcryl®90 is anticipated to attach dental dressings such as COE-PAK™ to the gum tissue and/or tooth enamel to assist in keeping dressings protected and intact for up to two weeks [6].
In the summer of 2011, GluStitch introduced PeriAcryl®90 High Viscosity, a thicker formulation to deliver additional control when applying. This novel product is 9 times denser as compared to the original PeriAcryl®90 formulation and has the identical strength and resilient characteristics that oral surgeons have come to depend on. Its features include biocompatibility, non-toxicity, rapid setting time, better visibility, and convenient usage [7]. Furthermore, it avoids wastage of time when compared to traditional sutures, and generally does not require follow-up. In dental practice, it has been consumed in numerous branches as post-extraction bandages and hemostatic materials, retrograde restorative materials, etc. Butyl esters offer durable bonds and are firm [8].
PICO question
P: Patients underwent intraoral surgeries.
I: Cyanoacrylate
C: Collagen
O: Quicker wound healing with better patient satisfaction
Aims of the study
The purpose of this systematic review was to compare cyanoacrylate and collagen when it comes to successful intra-oral wound healing.
Materials and Methods
Using the databases PubMed, Medline, and ScienceDirect, a comprehensive evaluation of the literature from 2012 to 2023 was conducted. The keywords used were “cyanoacrylate”, “collagen”, and “wound dressing”. The method of selecting the articles that were searched for was shown in a PRISMA flowchart (Figure 1).
The following requirements must be met for inclusion:
Exclusion criteria
|
|
|
Figure 1. PRISMA Flow Diagram |
Risk of bias assessment
The efficacy of the included studies was evaluated using the Cochrane risk of bias assessment technique, which included selection bias in randomization, concealment, binding as well as reporting of outcomes (Table 1).
Table 1. Summary of Cochrane Risk of Bias Assessment
|
Study |
Selection Bias/Appropriate control selection/baseline characteristics similarity |
Selection bias in randomization |
Selection bias in allocation concealment |
Performance-related bias in blinding |
Reporting bias/Selective reporting of outcomes |
Detection bias Blinding outcome assessors |
Accounting for confounding bias |
|
Mendoza-Azpur et al. (2021) [6] |
+ |
+ |
+ |
+ |
- |
+ |
+ |
|
Basma et al. (2023) [9] |
+ |
- |
+ |
+ |
+ |
+ |
+ |
|
Tavelli et al. (2019) [10] |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
As et al. (2018) [11] |
+ |
+ |
- |
+ |
+ |
+ |
+ |
|
Nevins et al. (2018) [12] |
+ |
- |
+ |
+ |
+ |
+ |
+ |
|
Thoma et al. (2012) [13] |
+ |
+ |
+ |
+ |
+ |
+ |
- |
|
Vastani et al. (2013) [14] |
+ |
+ |
+ |
+ |
+ |
+ |
- |
|
Sharma et al. (2019) [3] |
+ |
+ |
- |
+ |
+ |
+ |
+ |
Results and Discussion
The study by Mendoza-Azpur et al. (2021) sought to demonstrate the in vitro effectiveness of tissue adhesive based on cyanoacrylate and to assess clinically the healing of recently extracted sockets using adhesives applied to an exposed collagen membrane to maintain the alveolar ridge [6]. The alveolar bone was preserved using a resorbable collagen membrane that was purposely left exposed and a mineralized cortical allograft bone replacement. The exposed membrane was covered with a barrier made of Periacryl® 90 HV. The adhesive's biocompatibility was assessed using the EHS and EHIof perialveolar tissues at 12, 30, and 60 days after surgery. Periacryl® 90 HV cells were shown to have reduced cell viability as compared to cells without adhesive treatments. Periacryl® 90 HV was administered to perialveolar tissues, and no postoperative complications were seen.
Basma et al.'s research from 2023 evaluated the impact of four common wound dressings on PROMS after the extraction of free epithelialized mucosal grafts (FEGs). During the 14-day observation period, the patient's activity tolerance, desire to retreat, edema and bleeding levels, the number of analgesics taken, need for further analgesics, and severity of pain were all assessed using the visual analog scale. There were no statistically significant differences in the amount of edema, activity tolerance, or daily bleeding among the four groups. Out of all the groups, the PS was the least uncomfortable (over the 14 days). Graft thickness, graft length, graft width, or palatal thickness did not affect patient morbidity (P > 0.05).
To lessen postoperative pain after the harvesting of epithelialized gingival grafts (EGG), Tavelli et al.'s (2019) study evaluated the effects of hemostatic collagen sponge and collagen sponge bonded with a bio-adhesive material on the palatal donor sites [10]. The present study employed 44 EGGs obtained from 44 people. The test group received additional cyanoacrylate, whereas the control group had a hemostatic collagen sponge covering the palatal incision. A visual analog scale was used to evaluate the patient's level of discomfort after a 14-day observation period. There were statistically significant differences in pain intensity between the test and control groups on each study day (p= 0.01). Less analgesic was taken by the test group (p= 0.01). Pain was shown to be correlated with graft width smaller than 14 mm (p= 0.01).
This clinical study, evaluated by As et al. (2018), looked at how different hemostatic techniques influenced patients' pain after palatal gingival tissue harvesting [11]. The study involved the recruitment and random assignment of fifty patients who underwent mucogingival surgery involving the harvesting of gingiva grafts. Two weeks after surgery, patients rated their reported pain, degree of healing, usage of medicine, and willingness to repeat therapy using a visual analog scale (VAS). Notably, throughout the 14 days, the group treated with cyanoacrylate and gelatin sponge had very little pain. On day 10, the control group had the lowest healing scores compared to the other four test groups.
Nevins et al. (2018) conducted a clinical experiment to assess cyanoacrylate tissue glue's capacity to expedite the healing of extraction wounds requiring regenerative therapy in both soft and hard tissues [12]. Five extraction sockets, on the other hand, were not treated with tissue adhesive and were allowed to mend utilizing the secondary healing intention. The morphology of the bone surface and the color and form of the soft tissues were the main factors used to evaluate the results. It was better to use cyanoacrylate tissue glue as a defensive mechanism rather than an exposed collagen barrier membrane.
In comparison to spontaneous healing, the research by Thoma et al. (2012) evaluated whether collagen matrix (CM) improves early wound healing and aesthetics and decreases wound sensitivity [13]. Fifteen participants had 6-mm punch biopsies obtained in both palatal sites. While the other area (control) remained untreated, one location was given a CM. Measurements were also made of the remaining defect area, the color corresponding to surrounding tissue, and somatosensory traits at various times (pre-operative, postoperative, 4, 8, 15, and 29 days). The faulty area gradually shrank as a consequence of both treatments. Re-epithelization was completed in every instance by day 15. Day 4 (p = 0.05) and Day 8 (p = 0.01) saw a significant decrease in the defect area for CM. On days 4, 8, and 29, CM's color match was improved (p > 0.05). Day 4 somatosensory assessments revealed that CM's wound sensitivity was somewhat lower than the control's.
Vastani et al. (2013) evaluated the research to compare the histologic and clinical recovery of intraoral wounds closed with No. 3-0 silk sutures to wounds treated with isoamyl 2-cyanoacrylate glue [14]. Alveoloplasty was performed on thirty samples with edentulous arches in the mandibular anterior region; the length of the incision in each instance was the same as the distance from the midline. While No. 3-0 silk suture was utilized to close one side, the other was sealed with isomethyl 2-cyanoacrylate. The sutured side had more discomfort and erythema on the first, 7th, and 14th postoperative days; on the 21st postoperative day, it was similar to the glued side.
In this study, Sharma et al. (2019) compared the properties of wound healing between a collagen dressing that is sold commercially (CollaCote®) and a platelet-rich fibrin (PRF) membrane used as a palatal bandage [3]. While the second experimental group's palatal wounds were covered with PRF membrane, the first experimental group's ten patients' palatal wounds were coated with CollaCote® membrane. A visual analog pain rating scale was used to document the pain on the day of surgery as well as the seventh, twelfth, eighteenth, twenty-fourth, and thirtieth days after the procedure. When comparing the two groups' wound healing metrics to those within the groups, significant improvements were seen. In terms of size, depth, bleeding, pain, and epithelialization, there was no statistically significant difference between the groups; however, the PRF group healed more rapidly (Table 2).
Table 2. Summary of all included studies
|
Author’s name |
Objectives |
Patients |
Healing Material /method |
Follow-up period (days) |
Results |
|
The present study sought to demonstrate the tissue adhesive based on cyanoacrylate's effectiveness in vitro, as well as assess the adhesive's clinical usefulness in repairing recently extracted sockets. |
10 |
Periacryl® 90 testing |
12, 30 and 60 days |
The application of Periacryl® 90 HV to perialveolar tissues caused no postoperative complications. |
|
|
This study evaluated the impact of four common wound dressings on PROMS after the extraction of free FEGs. |
72 |
CPC+PRF + sutures PS |
14 days |
Out of all groups, the PS was least uncomfortable during 14 days. |
|
|
The study's goal was to find out how hemostatic and bio-adhesive-sealed collagen sponges affected the palatal donor sites. |
44 |
two collagen sponges: one sealed with bio-adhesive material |
14 |
There were significant differences in pain intensity between the test and control groups (p= 0.01). |
|
|
As et al. (2018) [11] |
This clinical study looked at how different hemostatic techniques affected the pain that patients felt after having palatal gingival tissue removed. |
50 |
1) sutures (2) cyanoacrylate (3) periodontal dressing (4) gelatin sponge |
14 |
The gelatin sponge and cyanoacrylate group exhibited little pain (VAS 0.5 points) over 14 days. |
|
Nevins et al. (2018) [12] |
The author's goal in doing this research is to determine whether, in comparison to spontaneous healing, CM improves early wound healing and aesthetics and decreases wound sensitivity. |
25 |
Cyanoacrylate tissue adhesive and collagen matrix |
|
Cyanoacrylate tissue glue was better than collagen barrier membranes for protection. |
|
Thoma et al. (2012) [13] |
This clinical study looked at how well cyanoacrylate tissue adhesive works at speeding up the healing of wounds from tooth extraction. |
15 |
collagen matrix |
15 |
Day 4 somatosensory assessments demonstrated somewhat lower wound sensitivity for CM than the control. |
|
The purpose of this study is to evaluate the efficacy of isoamyl 2-cyanoacrylate glue vs No. 3-0 silk suture for the healing of intraoral lesions. |
30 |
isoamyl 2-cyanoacrylate glue |
first, seventh, fourteenth, and twenty-first postoperative days |
On the seventh postoperative day, only the sutured side's vascularity was higher than on the fourteenth. |
|
|
This study compared the wound-healing properties of a commercially available collagen dressing to those of a platelet-rich fibrin (PRF) membrane employed as a palatal bandage. |
20 |
CollaCote® dressing, and PRF membrane.
|
7th, 12th, 18th, 24th, and 30th postoperative days |
Both groups showed significant wound healing improvements compared to within groups. |
The outcomes of this research provide evidence in favor of the use of cyanoacrylate as the preferred material for intraoral wound healing. In a recent study conducted by Mansoor et al. (2022), it was shown that the introduction of Periacryl® 90 HV tissue glue to a cell culture medium resulted in a significant decrease in cell viability [15]. There are two potential reasons for this behavior seen in the anionic polymerization of cyanoacrylate molecules. One of the primary concerns associated with the polymerization process is the occurrence of an exothermic reaction, which has the potential to elevate the temperature of the surrounding tissues. Another noteworthy aspect is the production of breakdown products, namely cyanoacetate, and formaldehyde, as a result of the reaction.
Cyanoacrylates exhibit efficacy in site management and hemostasis because of their dual properties of bacteriostasis and hemostasis. Cyanoacrylates have been used to achieve many therapeutic outcomes, including the management of extraction sockets, stability of mandibular fractures, facilitation of intraoral wound healing, repair of facial esthetic grafts (FEGs), and promotion of periodontal flap healing. According to Raj et al. (2022) and Stavropoulou et al. (2019), it has been shown that cyanoacrylates exhibit less inflammation and a more homogeneous presence of neutrophils, lymphocytes, histiocytes, and eosinophils compared to sutures [16, 17]. These data also corroborate the outcomes of our investigation.
The present investigation demonstrated that the use of a collagen sponge in conjunction with cyanoacrylate bio-adhesive applied over the palatal incision resulted in a much greater reduction in pain perception subsequent to EGG surgery compared to the use of a collagen sponge alone (p = 0.01). Cyanoacrylate has been used for a diverse range of applications, such as the application of periodontal dressing, the sealing of sinus membrane perforations, the stabilization of bone fragments during fracture treatment, and the closure of peripheral nerve anastomosis inside the mouth cavity [18].
While some authors have recommended oral wound protection with a hemostatic agent, adding an adhesive compound on top of a hemostatic one may strengthen wound covering and reduce post-complication, which was previously believed to be related to wound healing by secondary intention. Because of its strong sealing, bacteriostatic, and hemostatic qualities, cyanoacrylate can heal palatal wounds [19].
According to a study, the palatal covering may promote faster palate wound healing and lessen patient discomfort. In particular, the best technique for treating palatal wounds seems to be DLP with cyanoacrylate glue used over a hemostatic collagen sponge [20]. The barrier membrane over the graft may be covered and protected without moving it using cyanoacrylate tissue glue. It is crucial to utilize it responsibly to avoid the substance warping the soft tissue [21].
Many studies have been conducted on butyl and octyl cyanoacrylates, focusing on skin applications [22-24]. Thus, evaluating their functioning in the context of the oral cavity was necessary. Inflammation and infection levels serve as the strongest indicators of healing. Tenderness and erythema are the clinical manifestations of inflammation seen. In the first seven postoperative days, the cyanoacrylate adhesive site had a lower inflammation; however, between the 14th and 21st postoperative days, the inflammatory reaction was the same in both instances [25].
Conclusion
Using cyanoacrylate tissue adhesive as a wound healing agent instead of an exposed collagen barrier membrane was found to be superior. They are effective for site management and hemostasis because they have both bacteriostatic and hemostatic qualities. Cyanoacrylates were discovered to have less inflammation and a more uniform distribution of neutrophils, lymphocytes, and eosinophils than sutures.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None