The Coronavirus Disease 2019(COVID-19) virus testing can be done using multiple specimen types, mainly nasopharyngeal, saliva, and serum. The nasopharyngeal swab (NPS) is a gold standard in COVID-19 testing and diagnosis but is often uncomfortable for the patient and requires professional expertise in sample collection. The rationale of this study was to evaluate saliva, nasopharyngeal, and serum detection of COVID-19 and compare saliva with other specimens in COVID-19 testing. Using PRISMA 2020 guidelines, a data search was performed in the PubMed, Saudi Digital Library, and Cochrane COVID-19 study register. QUADAS 2 tool was applied to assess the quality of the studies included. The efficacy of saliva, serum, and nasopharyngeal specimens was the primary outcome measured in terms of sensitivity and specificity, and the secondary outcome was the comparison of saliva with NPS and serum for COVID-19 detection. Data were extracted from 39 studies-20 countries- 20,024 patients and 22123 samples. QUADAS-2 tool was applied. Meta-analysis showed significant differences in sensitivity between all specimens and when NPS is compared to saliva. Within the limitations, despite a significant heterogeneity (P < 0.001), the efficacy in the detection of COVID-19 is more in a balance between saliva and NPS. Saliva-Area under the curve (AUC) = 0.97, nasopharyngeal specimen (NPS): AUC= 0.94, AUC=l.00, suggestive of an excellent performance of serum (active infection)>saliva>NPS specimen in SARS- CoV-2 detection. The study's outcomes suggested that saliva specimens can be used as a non-invasive diagnostic method in COVID-19 testing.
Introduction
COVID-19 is a coronavirus disease which was first identified in Wuhan city in China in December 2019 [1]. This viral infection is caused by a novel coronavirus identified as Severe Acute Respiratory Syndrome Coronavirus 2 abbreviated as SARS- CoV-2 [1, 2]. On March 11th, 2020, the COVID-19 outbreak was declared a pandemic by the World Health Organization(WHO) and is currently an ongoing pandemic with records of the second and presumed third wave [1-3]. As of February 21st, 2023, the cases recorded with WHO are 757,264,511 cases of confirmed COVID-19, including 6,850,594 deaths [4].
The main modes of transmission of the virus are through salivary droplets or respiratory droplets and close contacts. Aerosol and fecal-oral transmissions are also prevalent. Other routes of spread are through contaminated surfaces and fomites [1, 3, 5-10].
Despite nasopharyngeal swabs (NPS) being the gold standard in diagnosis, correct sampling is crucial and can be performed solely by trained professionals. This collection technique imposes an economic burden on healthcare systems in addition to logistic issues. Moreover, NPS specimen collection is contraindicated in patients with coagulopathy anticoagulant therapy and significant nasal septum deviation [11]. Clearly, there is a need for a simpler and less invasive method that also reduces the risk to healthcare personnel [12-16].
Since the presence of antibodies against SARS-CoV-2 has also been detected in saliva, saliva-based testing can be explored as an alternative sampling technique other than being a non-invasive, rapid test for COVID-19 [17]. There are several studies conducted on diagnostic reliability and comparison of saliva, nasopharyngeal, and serum-based COVID-19 tests [1, 5, 16].
There is a need to compare the effectiveness of these modes of COVID-19 testing in general, and it is important to evaluate the applicability concerns in dental settings for the prevention and detection of COVID-19 [18]. Therefore, the rationale of the study was to evaluate saliva, nasopharyngeal, and serum detection of COVID-19 detection and suggest the best possible patient-acceptable method with good diagnostic reliability among nasopharyngeal, saliva, and serum specimens. Hence, the current systematic review aims to evaluate the effectiveness of saliva-based diagnostic tests compared to nasopharyngeal swab-based and serum-based tests for detecting SARS-CoV-2.
Materials and Methods
This study was registered, and ethical committee approval was given to conduct the study.
PICO focused question
Are saliva-based tests comparable to nasopharyngeal and serum-based diagnostic tests?
PICO framework for focused question
Population- Patients screened/suspected or confirmed with Covid 19
Intervention -COVID-19 diagnostic test using saliva/NPS/Serum specimens
Comparator/control-RT PCR-based validatory tests
Outcome- sensitivity and specificity of each specimen-saliva/NPS/Serum
Data extraction
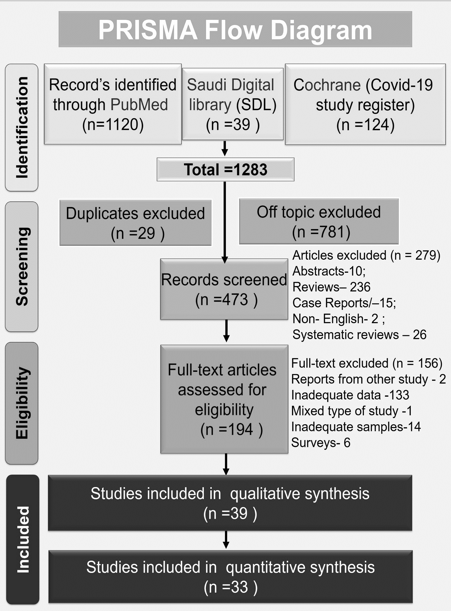
Data extraction was performed from three databases viz., PubMed, Saudi Digital Library, and Cochrane COVID-19 study register using the filter 'covid-19', 'SARS-CoV-2', 'saliva,' 'nasopharyngeal,' 'serum,' 'COVID-19 testing'. The present study was conducted per the PRISMA guidelines 2020 (Preferred Reporting Items for Systematic Reviews and Meta-analyses) [19], where data was extracted from databases and study registers from January 2020 to June 2021 (Figure 1).
|
|
|
Figure 1. PRISMA 2020 for database and registers combined to represent the data search, screening, eligibility, and inclusion of studies for systematic review and meta-analysis. |
Eligibility criteria
Exclusion criteria: duplicate and off-topic articles, non-English articles, abstracts, surveys, case reports, reviews, systematic reviews, and meta-analyses.
Inclusion criteria: Studies that explicitly assessed saliva, nasopharyngeal, and serum samples from patients screened/suspected/infected with SARS-CoV-2, full-text articles published in English, inadequate samples with less than 50 patients, reports extracted from another study, mixed type of studies combined with questionnaire and review and inadequate data.
Main outcomes
The efficacy of each of these specimen types, viz., the saliva, serum, and nasopharyngeal specimens, was the primary outcome measured in terms of sensitivity and specificity, and the secondary outcome was the comparison of saliva with NPS and serum for Covid 19 detection.
Risk of bias in individual studies
QUADAS 2 tool [20, 21] was used to test the quality of the included studies by assessing the risk of bias and the applicability concern. All the investigators were oriented and calibrated by experienced specialist dentists who have performed similar projects. While the studies were scrutinized for quality and inclusion, any disagreement among the investigators was mutually discussed and clarified, and an agreement was reached [20].
Patients: Asymptomatic or symptomatic patients with covid19 disease
Index test(s): Saliva/ NPS / serum specimen analysis to detect covid 19
Target condition: Patients screened for /suspected of/infected with COVID-19
Reference standard: RT-PCR (Reverse Transferase Polymerase Chain Reaction nucleic acid assay)
All four domains of risk of bias assessment and all three domains of applicability concerns were applied with custom-tailored questions to enable efficient assessment. If all signaling questions for a domain were answered 'yes,' then it was judged as a 'low' risk of bias, represented by a 'green' color. If any signaling question is answered 'no,' this flags the potential for bias and can be judged as a 'high' risk of bias represented by the color 'red.' Whereas, if any signaling question pointed to 'insufficient data' reported to permit a judgment, it was judged as 'unclear' represented by a 'yellow' color. While assessing three domains of applicability, the concerns were evaluated as 'Low/High/Unclear,' similar to the aforementioned method.
Results and Discussion
From the data retrieved using PRISMA 2020 guidelines (Figure 1), a total number of 1283 articles were collected. One thousand one hundred twenty articles were from PubMed, 39 were from the Saudi Digital Library (SDL), and 124 were from the Cochrane COVID-19 study register. Twenty-nine duplicate articles and 781 off-topic studies related to COVID-19 but not related to COVID-19 testing or the specimens under investigation were excluded from both databases and study registers. Articles under exclusion criteria, such as abstracts, case reports, non-English articles, reviews, and systematic reviews and /or meta-analyses, accounted for a total of 279 articles. Further, 194 articles were scrutinized for eligibility to be included in the current study. After a detailed review based on inclusion criteria, 39 studies were included for quality assessment, and 6 articles were included for quantitative synthesis, as detailed in Figure 2.
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
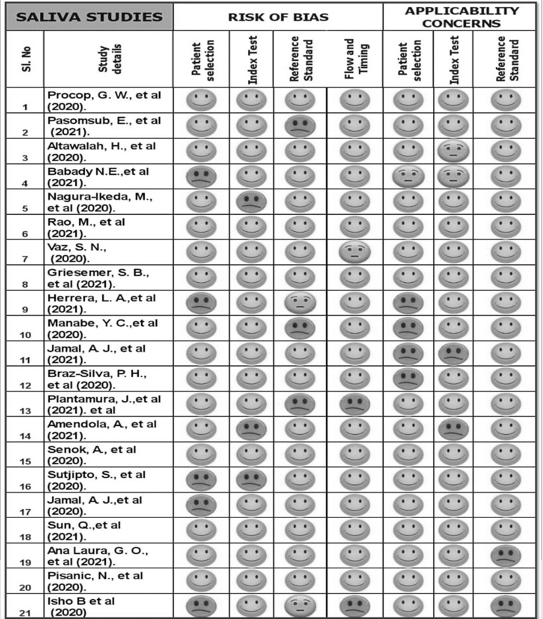
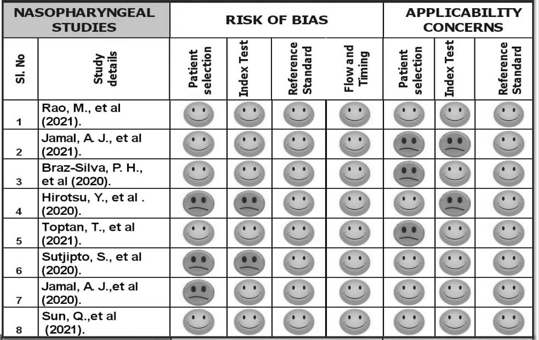
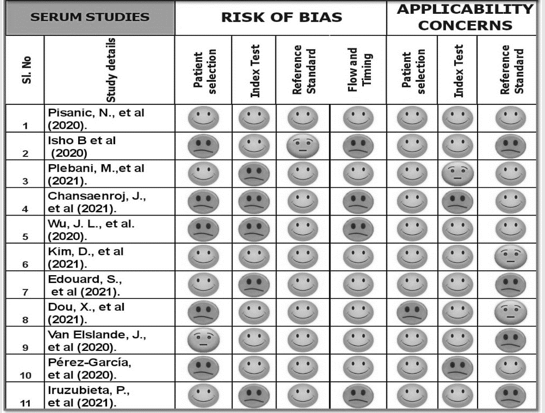
Figure 2. (a,b,c): representing the result of the quality assessment of the studies with the use of the QUDAS 2 tool on saliva 2 a), nasopharyngeal 2 b), and serum 2 c) based specimens, respectively. The yellow color represents the unclear risk of bias or applicability concern; the red color represents the high risk of bias and applicability concern; and the green color represents the low risk of bias and applicability concern. |
For the systematic review, 39 articles were assessed from 20 countries, 20,024 patients, and 22123 samples. Further quantitative assessments were performed on 33 articles that provided the percentage of sensitivity and specificity of the studied specimen.
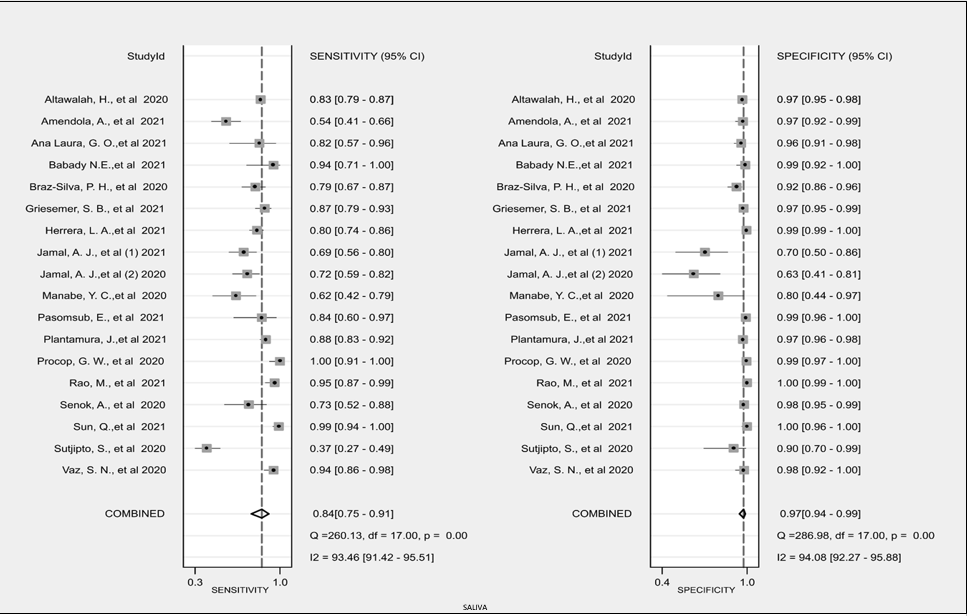
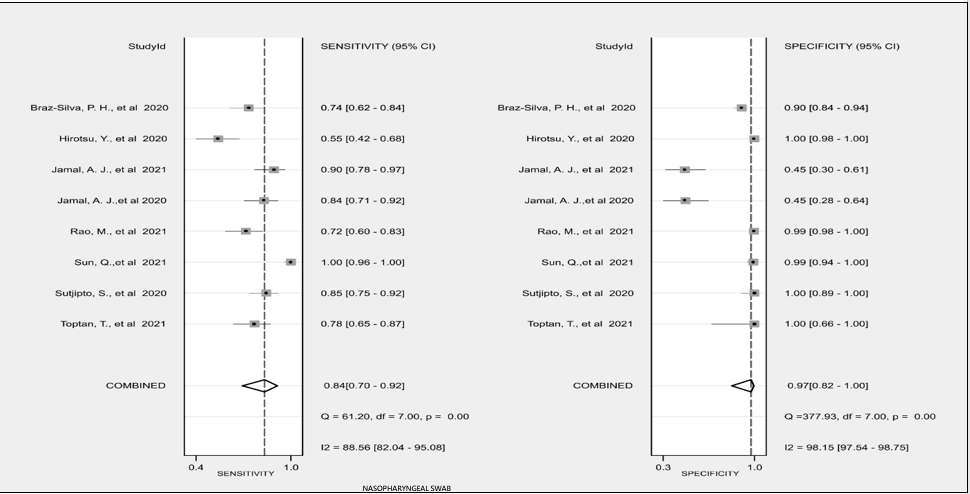
The details of sensitivity and specificity of the studies from saliva, nasopharyngeal, and serum specimens included in the meta-analysis are represented by forest plots, as shown in Figure 3. Table 2 shows the data on the performance of all three types of specimens under review. The positive likelihood ratio (PLR) and their respective 95%CI are above 1(>1). This indicates that patients with positive test results are more likely to be diagnosed with COVID-19. Saliva samples had a PLR of 32.0 [14.0, 73.2], meaning patients with positive saliva test results are 32 times more likely to test positive for COVID-19 than a healthy subject. Similarly, a negative likelihood ratio (NLR) of below 1 (<1) indicates that a patient with a negative test result is less likely to have COVID-19. A lower NLR specifies a smaller proportion of patients with COVID-19 who tested negative compared to those who tested negative for COVID-19 testing and are not infected with COVID-19. Therefore, patients with negative serum samples are substantially less likely to have a definite COVID-19 diagnosis (serum is the best-performing test in NLR). Additionally, the Diagnostic Odds Ratio (DOD) is the odds that the test yields positive results minus the odds of negative results. Again, serum testing yielded the highest DOD; thus, serum tests (during active infection and detected with IgG)are the best-performing screening tests.
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
Figure 3. Forest plots for the saliva studies, Nasopharyngeal (NPS) studies, serum studies |
Table 1 demonstrates the evaluation of base data such as true positive, false positive, false negative, true negative, and total cases.
Table 1. Statistical base data of studies included in metal analysis
|
Authors and Year |
TP |
FP |
FN |
TN |
Total |
|
Saliva |
|||||
|
Altawalah et al. (2020) [22] |
305 |
17 |
61 |
508 |
891 |
|
Amendola et al. (2021) [23] |
36 |
3 |
31 |
99 |
169 |
|
Ana Laura et al. (2021) [24] |
14 |
6 |
3 |
133 |
156 |
|
Babady et al. (2021) [25] |
16 |
1 |
1 |
69 |
87 |
|
Braz-Silva et al. (2020) [26] |
55 |
10 |
15 |
121 |
201 |
|
Griesemer et al. (2021) [27] |
91 |
10 |
14 |
348 |
463 |
|
Herrera et al. (2021) [28] |
139 |
10 |
34 |
1867 |
2050 |
|
Jamal et al. (2021) [29] |
44 |
8 |
20 |
19 |
91 |
|
Jamal et al. (2020) [30] |
46 |
9 |
18 |
15 |
88 |
|
Manabe et al. (2020) [31] |
18 |
2 |
11 |
8 |
39 |
|
Pasomsub et al. (2021) [32] |
16 |
2 |
3 |
179 |
200 |
|
Plantamura et al. (2021) [33] |
180 |
29 |
25 |
971 |
1205 |
|
Procop et al. (2020) [34] |
38 |
1 |
0 |
177 |
216 |
|
Rao et al. (2021) [35] |
62 |
1 |
3 |
496 |
562 |
|
Senok et al. (2020) [36] |
19 |
9 |
7 |
366 |
401 |
|
Sun et al. (2021) [37] |
84 |
0 |
1 |
90 |
175 |
|
Sutjipto et al. (2020) [38] |
31 |
2 |
52 |
19 |
104 |
|
Vaz et al. (2020) [39] |
67 |
2 |
4 |
82 |
155 |
|
NPS |
|||||
|
Braz-Silva et al. (2020) [26] |
52 |
15 |
18 |
131 |
216 |
|
Hirotsu et al. (2020) [40] |
32 |
1 |
26 |
254 |
313 |
|
Jamal et al. (2021) [29] |
44 |
23 |
5 |
19 |
91 |
|
Jamal et al. (2020) [30] |
46 |
18 |
9 |
15 |
88 |
|
Rao et al. (2021) [35] |
47 |
3 |
18 |
494 |
562 |
|
Sun et al. (2021) [37] |
84 |
1 |
0 |
90 |
175 |
|
Sutjipto et al. (2020) [38] |
62 |
0 |
11 |
32 |
105 |
|
Toptan et al. (2021) [41] |
45 |
0 |
13 |
9 |
67 |
|
Serum |
|||||
|
Chansaenroj et al. (2021) [42] |
187 |
19 |
5 |
164 |
375 |
|
Dou et al. (2021) [43] |
57 |
4 |
3 |
141 |
205 |
|
Kim et al. (2021) [44] |
127 |
0 |
3 |
100 |
230 |
|
Pérez-García et al. (2020) [45] |
58 |
0 |
32 |
161 |
251 |
|
Plebani et al. (2021) [46] |
4 |
4 |
1 |
207 |
216 |
|
Van Elslande et al. (2020) [47] |
261 |
4 |
0 |
99 |
364 |
|
Wu et al. (2020) [48] |
74 |
0 |
0 |
74 |
148 |
Table 2. Summary performance estimates.
|
Parameter |
Saliva |
NPS |
Serum |
|
Sensitivity |
0.84 [0.75, 0.91] |
0.84 [0.70, 0.92] |
0.97 [0.88, 1.00] |
|
Specificity |
0.97 [0.94, 0.99] |
0.97 [0.82, 1.00] |
0.99 [0.95, 1.00] |
|
Positive Likelihood Ratio |
32.0 [14.0, 73.2] |
28.0 [4.2, 189.4] |
72.2 [ 18.2, 287.4] |
|
Negative Likelihood Ratio |
0.16 [0.10, 0.26] |
0.17 [0.09, 0.32] |
0.03 [ 0.01, 0.13] |
|
Diagnostic Odds Ratio |
199 [58, 687] |
168 [22, 1281] |
2827 [410, 19476] |
The heterogeneity among the three specimens of saliva, NPS, and serum. The variation in the outcomes obtained by each study explained in terms of statistical heterogeneity, is depicted in Table 3. The null hypothesis is, 'all the studies have the homogenous outcome in COVID-19 testing for its detection of SARS CoV 2'. When the p-value of significance measured with the Chi-square test is more than 0.1(p>0.1), it would confirm the null hypothesis. However, as shown in Table 3, p<.0001 indicates heterogeneity among the outcomes of COVID-19 testing. Significant heterogeneity is obtained with an inconsistency index (I2) of > 50%. As shown in Table 3, there is substantial heterogeneity between studies across different tests, ranging between 96-99% with statistically significant p values.
Table 3. Heterogeneity statistics for the performance of Saliva, NPS, and Serum specimens for COVID-19 testing; NPS: nasopharyngeal swab.
|
Parameter |
Measure |
Saliva |
NPS |
Serum |
|
Heterogeneity |
Q |
44.639 |
153.041 |
70.838 |
|
df |
2.00 |
2.00 |
2.00 |
|
|
P(x2) |
< 0.0001 |
< 0.0001 |
< 0.0001 |
|
|
Inconsistency |
I2 [95%CI] |
96 [92 - 99] |
99 [98 - 99] |
97 [95 - 99] |
Fangan plots for saliva, NPS, and serum estimated how considerably the diagnostic test result using saliva, NPS, and serum changes the probability that a patient has COVID-19. Considering an initial probability of 25% for having a COVID-19 infection, results revealed that such a probability had increased to 91%, 90%, and 96% when saliva samples, NPS samples, and serum samples were positive for COVID-19. Additionally, the probability of COVID-19 has decreased from 25% to 5%, 5%, and 1% when saliva, NPS, and serum samples tested negative, respectively.
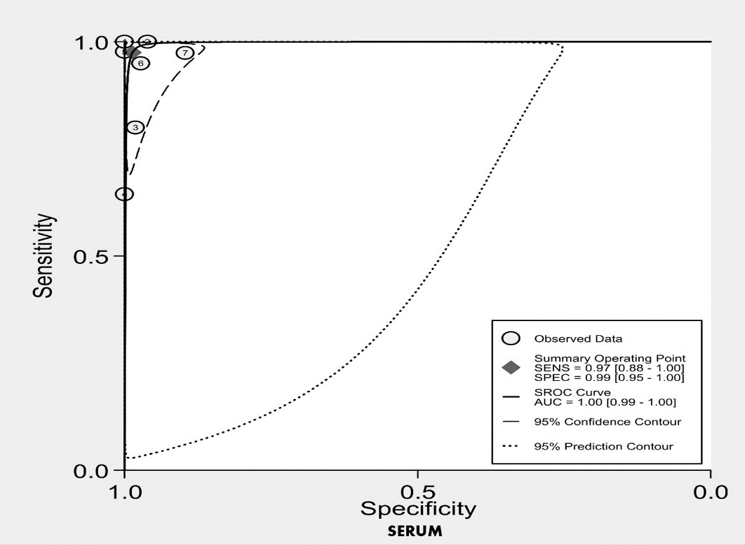
The Summary Receiver Operating Characteristic (SROC) curve - Area Under the Curve (AUC) (Figure 4) illustrates the pooled sensitivity of the three diagnostic tests under evaluation. ROC represents a probability curve for each specimen to detect COVID-19, and AUC signifies the measure of separability among these tests in COVID-19 diagnostic testing. Thus, the SROC curve-AUC model can help distinguish among the specimens for its capability to detect COVID-19. The pooled sensitivity of saliva tests was 0.84 (95% CI, 0.75 to 0.91), which indicates a good discriminative capacity of the test to detect SARS-CoV-2 positive cases, while the pooled specificity was 0.97 (95%CI, 0.94 to 0.99), which indicates a high performance of the test to discriminate COVID-19-negative patients. The AUC of saliva was 0.97 (95%CI, 0.95 to 0.98), suggesting an excellent performance of saliva tests in the detection of the virus.
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
Figure 4. Summary Receiver Operating Characteristic (SROC) curve - Area Under the Curve (AUC) for Saliva 5a, NPS 5b, and Serum 5c respectively |
The pooled sensitivity of NPS tests was 0.84 (95% CI, 0.70 to 0.92), which indicated a good discriminative capacity of the test to detect SARS-CoV-2 positive cases, while the pooled specificity was 0.97 (95%CI, 0.82 to 1.00), which indicates a high performance of the test to discriminate COVID-19-negative patients. The AUC of NPS was 0.94 (95%CI, 0.92 to 0.96), suggesting a very good performance of NPS tests in the detection of the virus.
The pooled sensitivity of serum tests was 0.97 (95% CI, 0.88 to 1.00), which pointed to a good discriminative capacity of the test to detect SARS-CoV-2 positive cases, while the pooled specificity was 0.99 (95%CI, 0.99 to 1.00), which indicates a high performance of the test to discriminate COVID-19-negative patients. The AUC of serum was 1.00 (95%CI, 0.95 to 0.98), suggesting an excellent performance of saliva tests in detecting SARSCoV2.
The results revealed that the highest detection efficacy was for serum samples (0.97, 95% CI, 0.88 to 1.00), followed by saliva samples (0.84, 95% CI, 0.75 to 0.91), and NPS (0.84, 95% CI, 0.70 to 0.92). Serum samples had also the highest pooled specificity estimate (0.99, 95% CI, 0.95 to 1.00). However, it has to be noted that the serum samples estimated carried out were in samples suspected of or infected with COVID-19 and who were detected to be positive for infection, representing the active infection stage. All studies assessed did not perform immunoglobulins IgG, IgM, and IgA levels. The data represented is of IgG levels, which showed the highest sensitivity, specificity, and detection.
The systematic review and meta-analysis were carried out to consider the reliability of saliva-based COVID-19 testing for screening or home-based remote testing, which does not require specimen collection by a trained professional. The study was also considered since saliva is a specimen routinely dealt with by dental professionals in daily dental practice. Hence, understanding the diagnostic accuracy of saliva is of utmost importance to dentists in particular. With this view, the three most commonly used specimen collection methods, viz., saliva, NPS, and serum, were analyzed for their diagnostic accuracy, and the individual specimen results were compared.
A nasopharyngeal swab, being a respiratory specimen, has been considered the gold standard specimen collection technique in SARS CoV-2 detection and has been widely used as a reliable tool in COVID-19 testing and retesting [22, 23, 26, 29-32, 34-38, 40, 41, 49, 50]. The studies that solely depended on nasopharyngeal specimens were less common [40, 41, 50-52]. A few factors may explain the reasons for limitations in the use of NPS despite being considered a preferred specimen. The viral load in NPS at different stages of COVID-19 can vary and may show lower scores in later phases or stages [53]. This can contribute to false-negative results [52, 54, 55]. The performance of the test may also depend on the high-quality samples collected, influenced by the patient's compliance with the instructions during specimen collection. Also, the inappropriate technique of specimen collection can lead to false negative results. Another observation regarding the NPS specimen was that the confirmatory test by trained professionals in an inpatient setting yielded more reliable results than the outpatient test carried out in suspected patients [52]. The NPS technique is less accepted among pediatric patients. This technique is recommended for pediatric patients with suspected COVID-19, presence of close contacts, and epidemiological factors like clusters of infection or hospitalization [56-60]. There are also multiple reports of its complications such as pain, fracture of the nasopharyngeal swab shaft and its dislodgement, swallowing of the fractured swab stick, and epistaxis, many of which required interventions for its removal [61-67].
Serum samples, on the other hand, could be investigated for the presence of various immunoglobulins (Ig). Ig A, IgG, and IgM levels were explored during various phases of disease activity and also compared with other specimens. These study results were indexed with RT-PCR analysis as a confirmatory test. The results of our study pointed out that Ig G was found to be more specific in symptomatic infected patients with covid 19 compared to asymptomatic patients and was shown to represent many reliable values during active infection [42-48, 68-71]. This can be explained based on the seroconversion period. Severe cases of SARS-CoV-2 infection have an earlier seroconversion to develop high SARS-CoV-2- 2 specific IgG levels in comparison to cases with mild symptoms. At times, measurable IgG antibodies may not be evident in serological analysis. However, in such cases, neutralizing antibodies to the virus may suggest immunity [72, 73]. The frequency and the time the serum samples were collected between the patients, as well as the uncertainty of accurate seroconversion time when the specific IgG response started, can be possible confounding factors in these studies. IgG levels for SARS-CoV 2 can be dependable as an adjunct aid in evaluating the status of active COVID-19 infection [74]. In contrast, serological analysis with suboptimal sensitivity levels and specificity levels for COVID-19 testing is not recommended as a confirmatory test [42-48, 68-73, 75-77]. It was also noted that the majority of these studies lacked a unified technique or methodology in the analysis for the standardization of serological specimens, which might have led to the underestimation or overestimation of the results.
Saliva can be a potential specimen for COVID-19 detection due to multiple reasons. Saliva contains epithelial cells shed from the oral cavity that have numerous Angiotensin-Converting Enzyme 2 (ACE2) receptors. ACE2 is critical for the entry of SARS-CoV-2 into the cells; hence, saliva is a good specimen that can help in COVID-19 testing. For dental practitioners, saliva is the most easily accessible specimen for outpatient screening or diagnosis of the patients, as well as healthcare workers within or outside the healthcare setup [78]. Since dental practice involves contact with saliva, direct or indirect transmission of SARS-CoV-2 is unavoidable, and dentists and allied dental professionals should take proper precautions [26, 79, 80]. On the other hand, saliva is the most easily accessible specimen in dental practice. Dental practitioners pose a high risk of exposure via saliva contamination from infected asymptomatic or symptomatic COVID-19 infected patients. At the same time, access to saliva-based tests can be very beneficial to prevent the spread of SARS-CoV-2 in dental setups.
Salivary SARS CoV- 2 can present via three routes: (1) liquid droplets from the lower and upper airway tract, (2) from gingival crevicular fluid sourced through SARS CoV 2 infected blood, and (3) salivary glands and its ducts [80, 81]. The ACE 2 inhibitor levels in COVID-19-infected patients are found to have higher levels in minor salivary glands in comparison to the lungs. This can explain the detection of SARS-CoV 2 in asymptomatic individuals even before the radiologic imaging features of lung involvement appear and also highlights saliva as a potential source of virus transmission [82]. Studies have reported the detection of COVID-19 among asymptomatic and symptomatic patients infected with COVID-19 [83-89]. Most of the studies follow any of these three approaches in the collection of saliva collection: using saliva swabs, coughing out the saliva, and direct collection from the duct of the salivary gland [90]. However, from the results of this study, it was observed that these collection techniques were not standardized, which might be a confounding factor affecting the results of these studies. Saliva was found to illustrate temporal fluctuations where peak levels in viral load were observed during the early days of symptom onset, and the values were found to decline later on [72, 91].
Saliva can be considered a potential alternative specimen for COVID-19 testing as NPS specimen collection can cause discomfort to the patient and a related risk of complications [92]. The requirement of trained professionals, personal protection equipment, and transport of the sample collection kits can be a logistic and economic burden impeding the nation's economic growth. The choice of self-collected saliva for large-scale screening using the proper collection technique can be a strategic way forward to resolve the aforementioned issues. Variations in test results with false negative nasopharyngeal sample results were noted among the professionally trained personnel, pointing to the need for internal standardization, calibration, and monitoring requirements for the NPS technique. Such instances have led to retesting, especially when symptoms were positive for COVID-19 [14, 93].
With the growing demand for testing and retesting and regulations worldwide for travel, quarantine, and screening purposes, saliva specimens stand out as a simple, non-invasive method for COVID-19 testing. With no procedural discomfort, no contraindications in medically compromised patients, accepted by children and adults, and comparable outcomes of the saliva and NPS tests, several studies advocate the use of saliva in the diagnosis of COVID-19 [7, 14, 26, 72, 79, 83-91, 93-105].
The study had a few limitations despite the large volume of data available for the specimens, especially NPS and saliva. There is a lack of synchronous methodology of detailed observations and statistical evaluations, which poses a great difficulty in retrieving the base data for performance analysis. There were multiple techniques and methodologies for the conduct of the test, which were not uniform and influenced the parameters analyzed in the study, even though the results were confirmed with RT-PCR, many of them being confirmed at different time intervals. Since there were several studies to compare the three specimens, saliva, NPS, and serum, for sensitivity and specificity, the results are generalizable. Serum specimen results are not generalizable due to insufficient studies, and the immunoglobulin estimation needs to be assessed in early and active infection. Within the limitations, despite a significant heterogeneity (P < 0.001), Saliva specimens had been found to provide good diagnostic efficacy in the detection of COVID-19 and can be used as an alternative reliable specimen in COVID-19 detection.
Conclusion
The result of our systematic review and meta-analysis concluded that the efficacy of saliva in the detection of COVID-19 is reliable, and results can be comparable to the gold standard- Nasopharyngeal specimen. NPS specimens should be collected with caution by trained professionals to avoid complications and accurate diagnosis. Serum specimens for SARS CoV-2 specific IgG are a good method of active COVID-19 testing in comparison to saliva and NPS specimens in symptomatic COVID-19 infected patients. However, it should not be used solely as a diagnostic test.
The saliva specimen collection technique is non-invasive and easy to perform. It does not require trained professionals, which will provide good patient acceptance and be safe to perform on children. Saliva-based COVID-19 testing can be self-administered. At-home or chair-side evaluation with test kits can be of ease, especially in the geriatric population and medically compromised patients, including patients on anticoagulants, and are promising specimens for point-of-care diagnostics. Saliva-based testing can be performed at ease by dental health care practitioners without referring a patient or employee for COVID-19 testing if proper personal protection precautions are taken. Also, it has high potential to be employed for wide-scale testing, especially in educational, business, social, and entertainment sectors, while we return optimistically to post-pandemic normalcy in life.
Future studies should consider standardization of techniques such as validation of the best technique using saliva specimens for COVID-19 testing and analysis of results for good diagnostic reliability. From the results of such a study, the best collection technique using point-of-care diagnostics using saliva should also be analyzed for diagnostic efficacy.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: This study was registered with the university research center with the ethical approval number IRB [SRP/2021147I455/447] for conducting the study.