Repairing and recreating injuries in the craniomaxillofacial area presents great difficulties because of the complex anatomy, individual features of every defect, and delicate character of the related systems. We present the case of a 20-year-old male patient admitted with an open fracture of the right zygomatic bone following a fall during the traditional Kyrgyz game of "Kok-boru." The patient sustained significant trauma resulting in facial asymmetry, an open infraorbital wound, and symptoms such as headaches, dizziness, and nausea. The radiographic evaluation confirmed a displaced fracture of the zygomatic bone. The complex nature of the injury required a multidisciplinary approach to achieve favourable reconstructive outcomes. This case emphasizes the essential importance of specialized and culturally sensitive trauma treatment in handling particular damage situations. The interaction of conventional cultural events with contemporary medical concerns highlights the need of customized approaches in controlling injuries connected to region-specific activities. Moreover, this study emphasizes the wider consequences of early and coordinated intervention in reaching positive reconstructive and functional results in craniomaxillofacial injuries.
Introduction
The psychological and physical condition of a patient can be considerably influenced by facial injuries. Restoring look and function as well as avoiding disfigurement, stigma, and reduced self-esteem and social functioning depend on effective, customized treatment [1]. A variety of stressful events can cause severe face injuries include falls, assaults, domestic abuse, animal bites, sports injuries and high-speed motor vehicle collisions. Often involving high-velocity forces, these events present major management difficulties because of their potential for morbidity and fatality [2]. Among these traumatic scenarios, extensive facial avulsion and degloving injuries—such as those sustained during a horse-riding accident in the traditional Kyrgyz game of "Kok-boru"—introduce complexities marked by airway compromise, profuse bleeding, soft tissue loss, and severe disfigurement [3]. Beyond only acute physical manifestations, the effects include long-lasting post-traumatic aesthetic alterations and functional limitations that can have significant psychological effects. Emphasizing the difficult nature of injuries related to the Kyrgyz game "Kok-boru," this case focuses on presenting and managing a patient with a left zygomaticomaxillary complex (ZMC) fracture and globe avulsion.
Case presentation
A 20-year-old male, presented to the Osh Interregional Clinical Hospital, Osh City, Kyrgyzstan on December 22, 2023, with an open wound and pain in the right infraorbital region, accompanied by headaches, dizziness, ringing in the ears, nausea, and general weakness. The injury occurred a day earlier, on December 21, 2023, at approximately 3:00 PM, when the patient fell from a horse during Kyrgyzstan’s traditional game "Kok-boru". He experienced a brief loss of consciousness but did not seek immediate medical care. The clinical procedures adhered to the ethical standards established by the institutional and/or national research committee, as well as the 1964 Helsinki Declaration and its subsequent amendments or similar ethical standards [4]. Written informed consent was obtained from the patient for publication of this case report and accompanying images. All identifying information has been anonymized to ensure patient confidentiality.
On examination, the patient had an open, lacerated-contused wound measuring 4 cm in the right infraorbital region with soft tissue damage extending to the upper eyelid. The patient displayed motor function by moving all four limbs against gravity. The facial contours were disrupted, and palpation revealed a fracture in the right zygomatic bone. Despite the extent of the injury, the dentoalveolar system was intact with no occlusal misalignment.
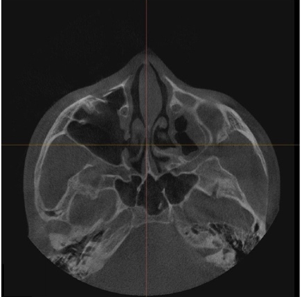
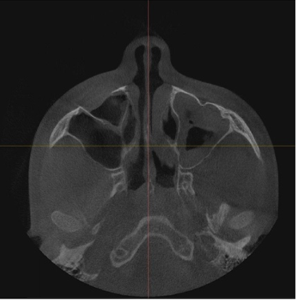
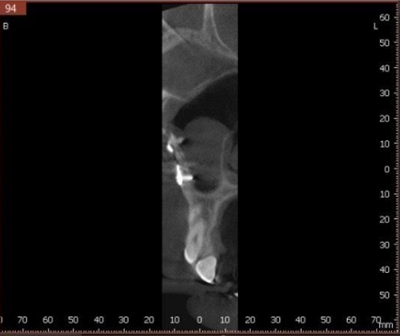
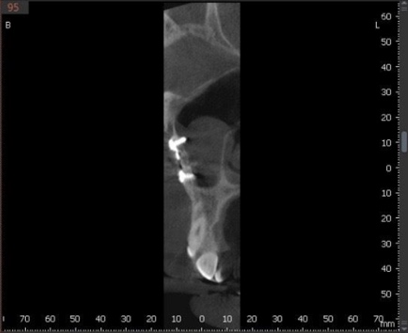
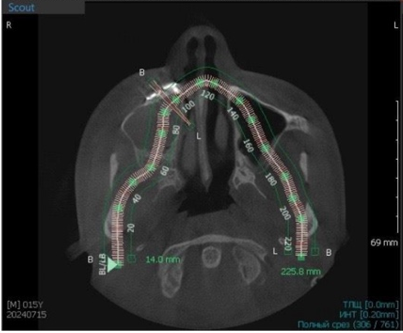
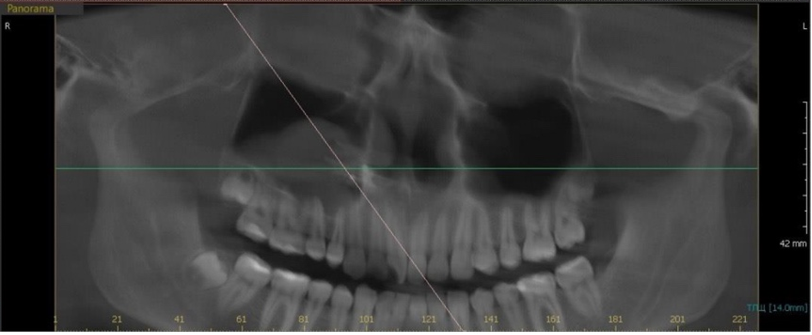
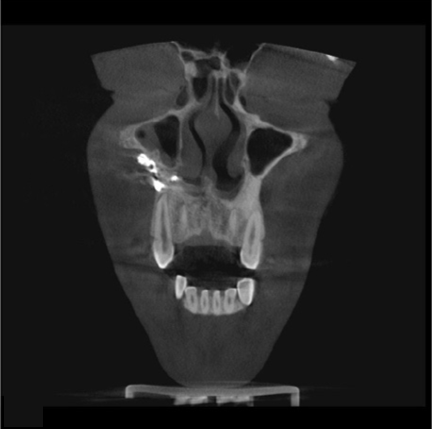
A radiographic study of the facial skeleton in frontal and lateral projections revealed on the right side fracture line including the maxillary sinus and infraorbital rim. Along with opacification of the maxillary sinus, lateral displacement of zygomatic bone fragments was noted, consistent with hematosinus—that is, blood accumulation within the sinus cavity. Although the intraoperative visualized skeletal view verified the presence of a fracture, the exact degree of the damage and the thorough assessment of bone fragment displacement called for advanced imaging modalities (Figure 1).
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
|
|
d) |
|
Figure 1. 3D X-ray imaging before surgery in various slices |
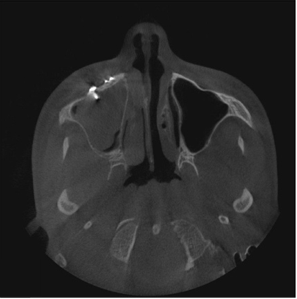
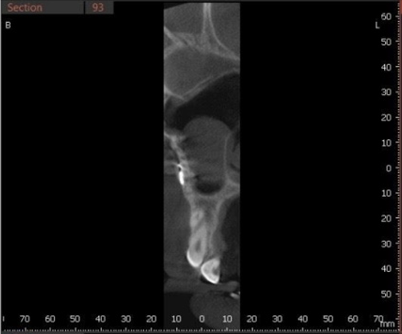
Axial and coronal views of computed tomography (CT) scans of the skull yielded a more finely detailed picture of the injuries. The CT Scan showed a zygomatic bone fracture with a corresponding injury to the right maxillary sinus (Figure 2). The existence of fluid buildup in the sinus indicated hemosinus. Mild displacement of the zygomatic bone was also observed, which caused disturbance of the usual anatomical outlines and compression of surrounding soft tissues. Examining the nasal mucosa revealed major damage including signs of mucosal rips and thickening. These results highlight the need for CT for the thorough evaluation of complicated maxillofacial damage.
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
Figure 2. 3D imaging of the skull base |
Materials and Methods
The surgical process started with many preparatory steps to create the right environment for the intervention. To be comfortable, the patient was given general anesthesia, and the environment was controlled during the process. Some of the antibiotics that are given prophylatically prior to surgery include; amoxicillin/clavulanate or ceftriaxone to help prevent perioperative infections. To minimize the risk of bleeding, hemostatic measures were taken appropriately. Preoperative diagnostics, X-ray & CBCT imaging were done to optimize the surgical approach and enhance the accuracy of fixation to the fracture site (Figure 3). The main surgical surgery followed a thorough and slow course. An incision at the sub-tarsal level—just below the lower eyelid—was used to reveal the fracture site. This allowed direct vision and zygomatic bone, orbital floor, and infraorbital rim manipulation. Pathologic elements including clots, bone spicules, and damaged mucosa could be removed in the maxillary sinus. The surgical field was made sterile by antiseptic irrigation with medications, such as gentamicin and betadine, therefore preventing infection.
|
|
|
|
a) |
b) |
|
|
|
|
c) |
d) |
|
|
|
|
e) |
|
|
Figure 3. Post-operative 3D imaging of the paranasal sinuses |
|
The reduction of bone fragments is to restore anatomical integrity and attain functional and aesthetic symmetry. The zygomatic bone and the front wall of the maxillary sinus were carefully repositioned, with intraoperative confirmation to ensure accurate anatomical alignment. The bone pieces were stabilized using titanium plates, each measuring 1.5–2 mm in thickness, affixed at several locations to improve stability and structural integrity (Figures 4a and 4b).
|
|
|
a) |
|
|
|
b) |
|
Figure 4. 3D post-operative imaging (a) lateral and (b) frontal views of the skull, with titanium fixation plates. |
These fixation devices offered substantial support for the reconstructed anatomical structure. The surgical site received multiple antiseptic applications before wound closure. Layered suturing of the mucosal, muscular, and dermal layers was executed to enhance healing and reduce scarring, hence ensuring functional recovery and aesthetic results. Post-fixation, wound. Debridement with gentamicin and Betadine wash was conducted, and closure was executed in layers. The last phase included post-fixation imaging which is used to assess the effectiveness of the surgical procedure. X-rays were used to ensure that the bones were well aligned and that the implants were in the right position to guarantee the proper alignment of the reconstructed structures (Figure 5). This step was important for assessing the results of the intervention and for defining any further therapeutic management that might be required.
|
|
|
a) |
|
|
|
b) |
|
Figure 5. X-ray of the skull post-surgery |
The patient was discharged 9 days after the surgery with well-planned postoperative management to enhance recovery and minimize complications (Figure 6).
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
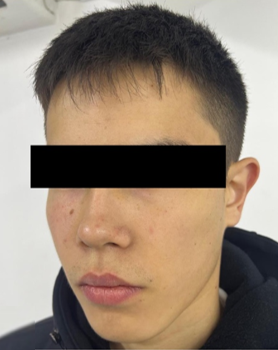
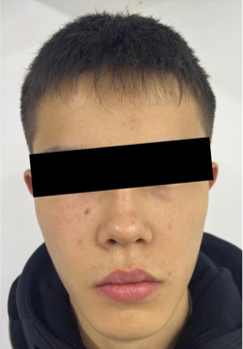
Figure 6. Postoperative gross view of the patient, a,b) View after 48 hours of surgery, c) A View on the first day after surgery |
Other than NSAIDs such as ibuprofen (600 mg) for analgesia and anti-inflammatory effect, the complete management plan also encompassed broad-spectrum antibiotics such as ceftriaxone, ciprofloxacin or amoxicillin/clavulanate to prevent infections. The use of nasal decongestant drops was also given to reduce edema and enhance drainage of sinuses. Cold compress was applied to the surgical site within the first 24 to 48 hours to help reduce swelling and hence improve the patient’s comfort and healing outcomes. After 7-10 days post-surgery, physiotherapy such as UHF therapy or magnetotherapy was started to promote tissue healing and to reduce inflammation. Within one to two weeks of follow-up, the clinical assessment and repeated radiographic examination to check on the anatomical alignment, the stability of fixation devices, and the general healing process. The patient exhibited satisfactory healing during the 2-week postoperative follow-up (Figure 7) [5-7].
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
Figure 7. Two-months postoperative picture from different face profile with (a), (b) and (c) showing satisfactory healing in patient |
The patient was given a personalized rehabilitation plan after surgery. As he healed, a prosthodontist suggested he fit a custom ocular prosthesis to restore facial aesthetics. Physical therapy kept his facial muscles toned and prevented atrophy. Visual rehabilitation improved his depth perception and field correction for monocular vision. He was advised to seek psychological assistance for his injury. He had regular follow-ups to check his recovery and adapt the treatment approach [5, 8-14].
Results and Discussion
Treating complicated hemifacial avulsion injuries requires a multidisciplinary approach and poses considerable therapeutic challenges. The biomechanics of the sport, which exposes players to a broad spectrum of trauma often affecting the stomach, chest, and head and neck areas, make the injuries suffered during "Kok-boru very unique [15]. If not properly controlled, at this age such accidents can cause long-term psychological and physical consequences [16-26]. Clinically, the face injuries resulting from "Kok-boru" differ greatly from those brought on by other types of trauma and call for different treatment approaches. To design and carry out the repair, this instance called for the coordination of radiologists, maxillofacial surgeons, and wound care experts. Addressing broad, linked facial avulsion and degloving wounds needed meticulous assessment and a tiered approach to give function restoration top priority along with cosmetic results top importance. The combined efforts of the multidisciplinary team made informed decisions and expert planning possible, therefore producing a good reconstructive result. Although the main repair restored the structural and functional integrity of the zygomatic bone, the patient's psychological recovery emphasizes the need to treat the emotional as well as the physical effects of such injuries [27-32].
Acknowledging both functional and cosmetic success in line with Rashid et al. (2020), early single-stage primary reconstruction clearly showed its importance [33]. Improving the likelihood of improved outcomes, reducing the danger of infection, and maximizing soft tissue rebuilding depended critically on immediate action inside damage. Ryan T. J. (2007) clarifies that dental management was attended to to avoid complications including hygiene and post-surgical care, such as maintaining the injured region sanitary and avoiding visiting dusty areas to avoid infection [34]. Ophthalmologists within the designated ideal timeframe focused especially on eyelid lacerations. Carefully repairing lacerations affecting the medial canthus, lacrimal, and tarsal glands was done to guarantee positive results through the complete closure of eyelid margins in layers as detailed by Moumita et al. (2023). As Holger et al. (2018) also show, radiological studies helped quite well during the intraoperative phase and post-operative follow-ups [35].
Conclusion
The effective treatment of complicated face damage resulting from the traditional Kyrgyz game "Kok-boru" is shown in this case report. The particular nature of the trauma needed a multidisciplinary approach for obtaining both functional and cosmetic rehabilitation efforts. This case highlighted the need for careful postoperative care to prevent complications and the significance of preserving original tissue viability during reconstruction, therefore influencing the management of similar challenging facial trauma situations. Increased awareness of the risks associated with traditional sports and the creation of preventive plans will help to lower the incidence of such injuries. Management of significant facial damage and guarantee of best results depend on specialized treatment and multidisciplinary cooperation.
Acknowledgments: The author extends sincere gratitude to the Osh Interregional Clinical Hospital and the Department of Maxillofacial Surgery for their invaluable support, resources, and expertise that greatly contributed to the successful completion of this study.
Conflict of interest: None
Financial support: None
Ethics statement: This study was conducted in strict adherence to the ethical principles outlined in the Declaration of Helsinki. Informed consent was obtained from all participants, and their identities have been anonymized to ensure confidentiality. Further details regarding the ethical protocols followed can be provided upon request by contacting the corresponding author.