FLUORIDE INDUCED CORROSION IMPACT ON PERI-IMLANTITIS: A SYSTEMIC REVIEW
Gintaras Janužis1, Greta Milvydaitė1, Miglė Miškinytė2*, Dominykas Latakas1, Gediminas Griškonis1
1Department of Maxillofacial Surgery, Lithuanian University of Health Sciences, Kaunas, Lithuania.
2Faculty of Odontology, Medical Academy, Lithuanian University of Health Sciences, Kaunas, Lithuania. [email protected]
https://doi.org/10.51847/ML9Ne75Wep
ABSTRACT
Dental implants primarily utilize commercially pure titanium (cpTi) and Ti-6Al-4V alloys, both boasting clinical success rates of up to 99% over a 10-year period. Regrettably, the surface of dental implants undergoes changes over time, and any alterations could trigger the onset of mucositis and peri-implantitis processes. This systematic review aims to evaluate the effect of fluoride and pH on titanium corrosion. A systematic review was conducted following the PRISMA guidelines. It included in vitro studies published in English that assessed the effects of various pH levels and concentrations of fluoride solutions on the corrosion of titanium disks. After conducting the initial search, our investigation yielded a comprehensive pool of data, amounting to a total of 358 publications. 6 studies met our inclusion criteria and were included. Titanium elution, surface roughness, discoloration, and change in gloss and open circuit potential (OCP) were analyzed. Studies showed that release of Ti ions, surface roughness and discoloration and gloss change increased as pH got lower and fluoride concentration got higher. OCP values decreased as the fluoride concentration increased and the environment got acidic. Hence, the interplay between pH and fluoride significantly influences titanium corrosion, with lower pH levels requiring less fluoride to initiate corrosion. This corrosion mechanism thus implicates periimplantitis as a potential consequence.
Key words: Fluorides, Corrosion, Periimplantitis, Titanium.
Introduction
Implant dentistry has emerged as a widely favored restorative solution in clinical settings. Titanium-based implants have been the primary choice for dental implant manufacturing since approximately 1981. The predominant alloys utilized include commercially pure titanium (cpTi) and Ti-6Al-4V, both demonstrating clinical success rates of up to 99% over 10 years [1]. The existence of a titanium oxide layer on the surface of the implant is regarded as crucial for titanium's biocompatibility, facilitation of osseointegration, and protection against corrosion of the titanium surface [2]. Unfortunately, the surface of dental implants changes over time, and if alterations occur, it could trigger processes such as mucositis and peri-implantitis [3].
Epidemiological studies conducted more than 70 years ago provided the basis for the use of fluoride in caries prevention [4]. The use of topical and systemic fluoride for oral health has made major reductions in dental caries prevalence and its associated disability [5]. According to ISO standards, the maximum fluoride content in toothpaste is 1500 parts per million [6] and fluoride varnish preparations can have a fluoride content of as high as 22,600 parts per million (ppm) [7]. Because fluoride toothpaste practically prevents caries, numerous individuals with titanium implants or prostheses in the oral cavity frequently utilize fluoride-containing toothpaste.
The corrosion behavior emerges as a critical determinant influencing the biocompatibility of metal implants, precipitating the liberation of metal ions, which may engender diverse detrimental outcomes [1]. While titanium alloys typically exhibit commendable corrosion resistance, this characteristic may be compromised under certain conditions, such as temperature fluctuations, pH variations, and alterations in the concentration of reactive ions (e.g., H+, Cl-, F-) [1, 8]. Hence, is it very important to understand if there is a significant negative fluoride impact and what factors induce those reactions. This study is designed to comprehensively investigate and analyze the effects of varying fluoride concentrations and pH levels on the corrosion behavior of titanium, aiming to provide a deeper understanding of the intricate interactions between these factors and their implications for the long-term stability and performance of titanium-based implants.
Materials and Methods
This systematic review adhered to the guidelines outlined in the Preferred Reporting Item for Systematic Reviews and Meta-Analyses (PRISMA) statement. Before commencement, a protocol was drafted and registered at PROSPERO, housed at the University of York's Centre for Reviews and Dissemination. The publication's distinct identifier for this protocol is CRD42023409747.
Clinical question
The clinical query was formulated in accordance with the Participant, Intervention, Comparison, Outcome (PICO) framework [9]. Do different pH and concentration fluoride solutions have an impact on titanium disk corrosion? (Table 1)
Table 1. Formulation of PICO question.
|
P (Population) |
Titanium disks |
|
I (Intervention) |
Titanium disk immersion into different pH and fluoride concentration solution |
|
C (Control) |
- |
|
O (Outcome) |
The evaluation of titanium disk corrosion: elution, surface roughness, discoloration, gloss change, open circuit potential. |
|
PICO |
Do different pH and concentration fluoride solutions have an impact on titanium disk corrosion? |
Inclusion criteria
Inclusion criteria include the following: In vitro studies published in the English language between 2014 and 2024; Fluoride concentration measured in ppm; pH impact on titanium corrosion was evaluated; Titanium alloys: commercially pure titanium (cpTi) or Ti-6Al-4V were used; At least one of the variables: titanium elution, surface roughness, discoloration and change in gloss or open circuit potential was evaluated.
Exclusion criteria
Exclusion criteria include letters, editorials, literature reviews, in vivo, animal studies, case reports, case series, systematic reviews, meta-analyses, and abstracts.
Search strategy and study selection
In accordance with the PRISMA guidelines [10], a rigorous electronic systematic literature search was independently undertaken by three researchers (G.M., M.M., and D.L.) across the databases PubMed, Science Direct, and the Cochrane Library. The search strategy incorporated specific keywords, including "fluoride," "fluorides," "fluoride ions," "corrosion," and "periimplantitis." The process comprised two sequential stages: an initial screening based on the titles and abstracts of publications, followed by a more comprehensive evaluation of the full-text articles that met the inclusion criteria identified during the first phase. Elimination of duplicate studies and those not aligning with the pre-defined inclusion criteria occurred at each stage. Selected articles underwent comparison, with any discrepancies resolved through researcher discussion. In instances where consensus was not achieved, consultation with seasoned researchers (G.G. and G.J.) was sought to facilitate consensus.
Risk of bias assessment
Three researchers (G.M., M.M., and D.L.) independently evaluated the risk of bias by utilizing the QUIN Tool (a quality assessment tool for in vitro studies) [11]. Discrepancies in their assessments were deliberated upon to achieve consensus. Should consensus prove unattainable through discussion, the expertise of a third-party consulting party (G.G. and G.J.) was enlisted to assist in resolving any discrepancies.
Results and Discussion
Study selection
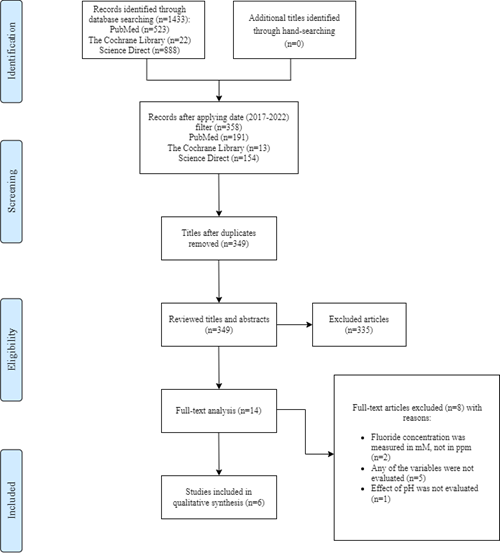
The depiction of the review process, encompassing articles, abstracts, and full-text publications, is presented through a PRISMA flow diagram (Figure 1).
|
|
|
Figure 1. Prisma flowchart. |
Characteristics of the included studies
6 studies were included in the qualitative synthesis. Overall, 5 studies used commercially pure titanium alloy (cpTi) [8, 12-15] and 2 studies used commercial titanium alloy (Ti-6Al-4V) [8, 16]. Fluoride concentration varied from 0,04 to 9000 ppm NaF and pH varied from 3 to 7,3. Corrosion was evaluated using a plasma spectrometer [12-15], scanning electron microscope [8, 14, 16], shape analyzer laser microscope [13], and electrochemical measurements were made [12]. The included articles were all in vitro studies published from 2014 to 2024 (Table 2).
Table 2. Characteristics of the included studies.
|
Titanium alloy |
Solutions |
Research method |
Investigated variables (+ yes, - no) |
||||
|
Elutet titanium |
Surface roughness |
Discoloration and change in gloss |
Open circuit potential |
||||
|
Huang et al. (2017) [16] |
Ti-6Al-4V |
solution A, pH 4.46/260 ppm fluoride; solution B, pH 4.41/178 ppm fluoride; solution C, pH 6.30/117 ppm fluoride; and solution D, pH 4.17/3.92 ppm fluoride); SALINE pH 6,24/3,56ppm fluoride |
field-emission scanning electron microscope (FE-SEM) |
- |
+ |
- |
+ |
|
Fukushima et al. (2017) [12] |
cpTi |
NaF solution (225 or 900 ppm F; pH 4.2 or 6.5) |
electrochemical measurements; plasma mass spectrophotometer |
+ |
- |
+ |
- |
|
Peñarrieta-Juanito et al. (2019) [8] |
cpTi and Ti-6Al-4V |
1.23% NaF (5,591ppm) pH 4 |
scanning electron microscope (SEM) |
+ |
+ |
- |
- |
|
Suzuki et al. (2019) [13] |
cpTi |
2% NaF (pH=7.3) and 9,000 ppm (pH=5.3) |
electron microscope; plasma spectrometer |
+ |
+ |
- |
- |
|
Chen et al. (2020) [14] |
cpTi |
A- HBSS; B- HBSS+0.04 ppm NaF (pH 7.3); C- HBSS+0.4 ppm NaF (pH 7.3); D - HBSS+0.04 ppm NaF (pH 5.0); E - HBSS+0.4 ppm NaF (pH 5.0) |
scanning electron microscope (SEM); plasma atomic emission spectrometer |
+ |
+ |
- |
+ |
|
Furiya-Sato et al. (2020) [15] |
cpTi |
artificial saliva, 1 M H2O2, 1 M H2O2 with catalase; 1000 ppmF pH=6.5; 1M H2O2 1000 ppm pH=6.5, 1M H2O2 9000 ppm pH 5.3. |
plasma mass spectrometer |
+ |
- |
+ |
- |
Risk of bias assessment
The visual presentation of the results derived from the assessment of bias risk is displayed below in Table 3.
Table 3. Risk of bias assessment using QUIN Tool. (Abbreviations: NA – not applicable)
|
Criteria Study |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
Final Score |
|
Huang et al. (2017) [16] |
2 |
0 |
NA |
2 |
2 |
0 |
NA |
2 |
0 |
0 |
2 |
2 |
60% |
|
Fukushima et al. (2018) [12] |
2 |
0 |
NA |
2 |
2 |
1 |
NA |
2 |
0 |
0 |
2 |
2 |
65% |
|
Peñarrieta-Juanito et al. (2019) [8] |
2 |
0 |
NA |
2 |
2 |
1 |
NA |
2 |
0 |
0 |
2 |
2 |
65% |
|
Suzuki et al. (2019) [13] |
2 |
0 |
NA |
2 |
2 |
2 |
NA |
2 |
2 |
0 |
2 |
2 |
80% |
|
Chen et al. (2020) [14] |
2 |
0 |
NA |
2 |
2 |
0 |
NA |
2 |
0 |
0 |
2 |
2 |
60% |
|
Furiya-Sato et al. (2020) [15] |
2 |
0 |
NA |
2 |
2 |
0 |
NA |
2 |
0 |
0 |
2 |
2 |
60% |
The criteria were assessed based on a scoring system as follows: Adequately Specified (Score=2), Inadequately Specified (Score=1), Not Specified (Score=0), and Not Applicable (NA). Upon computing the final score, results falling above 70% indicated a low risk of bias, while scores ranging between 50% and 70% indicated a medium risk of bias. Conversely, scores below 50% suggested a high risk of bias.
One of the included studies had a low risk of bias [13], and other studies had a medium risk of bias [8, 12, 14-16]. This situation arose because none of the studies provided a thorough explanation of sample size calculation or sufficiently addressed the blinding of outcome assessors. Furthermore, there was a lack of specification regarding operators and their training details in studies [14-16], or these details were inadequately addressed in studies [8, 12]. Additionally, no outcome assessor details were provided in studies [8, 12, 14-16].
Results of individual studies
The findings of individual studies were categorized based on the specific manifestations of titanium corrosion under investigation. Four groups of variables were formed: eluted titanium, surface roughness, discoloration, and change in gloss and open circuit potential.
Elutet titanium
Five of the studies examined the release of Ti ions [8, 12-15]. Studies by Suzuki et al. [13] and by Furiya-Sato et al. [15] showed that at an acidulate environment (pH=5.3) and 9,000 ppm significant titanium elution was present using cpTi (p<0.05). Furthermore, a study by Fukushima et al. [12] showed a rise in the elution of titanium following the immersion of titanium samples in NaF solution, particularly notable at low pH levels (pH=4.2), regardless of the NaF concentration (225 or 900 ppm) (p < 0.01). Chen et al. [14] found that the release of Ti ions increased statistically for both neutral and acidic groups. Generally, cpTi released a significantly higher amount of Ti ions at pH 5.0 compared to pH 7.3 (P<0.05). Peñarrieta-Juanito et al. [8] results revealed that the solution of 1.23% sodium fluoride had a high concentration of Ti, Al, and V metallic ions released. Mean values of the release of ions were lower for the hydrogen peroxide group with a pH of 7 compared to the F group (p < 0.05).
Surface roughness
Four studies examined surface roughness [8, 13, 14, 16]. The study conducted by Suzuki et al. [13] revealed that immersion in a NaF solution did not exert any discernible impact on the surface of titanium, with no observable corrosion occurring over a 7-day immersion period. Conversely, immersion in an acidulated phosphate fluoride solution (APF) with a concentration of 9,000 ppm and a pH of 5.3 resulted in significant surface roughening of the titanium due to corrosion within a mere 24 hours of immersion (p<0.05). Chen et al. [14] discovered that in neutral and acidic fluoride-free groups there were no localized corrosion pits observed, and the surface of cpTi disks appeared to be smooth. Micro pits appeared and increased in higher serum fluoride concentration. Exposure to fluoride in an acidic environment led to micro pit corrosion, which resulted in more significant and deeper consequences compared to exposure in a neutral environment. In the study conducted by Huang et al. [16], the findings indicated that Ti-6Al-4V samples exposed to solutions with elevated fluoride concentration and low pH exhibited a higher incidence of defects, notably including crevice corrosion and pitting, compared to other samples (p<0.05). A study by Peñarrieta-Juanito et al. [8] carried out that titanium alloys like Ti-6Al-4V are more prone to corrosion compared to commercially pure titanium when exposed to fluorides (p<0.05).
Discoloration and change in gloss
Two studies examined discoloration and change in gloss [12, 15]. Studies by Fukushima et al. [12] and Furiya-Sato et al. [15] point out that there were no notable post-immersion alterations in color or gloss observed in any of the commercially pure titanium samples, except in cases where they were subjected to treatment with acidic high-concentration fluoride solutions (specifically, 9000 ppm NaF at pH=5.3 and 900 ppm NaF at pH=4.2, respectively).
Open circuit potential
A reduction in the open circuit potential of a metallic material within a specific environment indicates heightened chemical reactivity and an increased susceptibility to corrosion Two studies investigated open circuit potential (OCP) [14, 16]. Both studies show that the OCP values of Ti-6Al-4V [16] and cpTi [14] gradually decreased as the serum fluoride concentration increased, which was more noticeable in solutions with lower pH levels.
The two most commonly used titanium alloys, cpTi and Ti-6A1-4V, have high osseointegration potential. They exhibit bioactivity and can promote bone formation upon direct interaction with their metallic surface [1]. Upon interaction with biological tissues, titanium develops an oxygen layer on its surface, a phenomenon that inhibits corrosion, rendering it an inert metal. Nevertheless, complete inertness in vivo is unattainable for any metal or alloy, as electrochemical processes can lead to the liberation of metal particles after interaction with interstitial fluids. Although the titanium oxide layer possesses regenerative capabilities, continual abrasion and exposure to chemical agents such as acidic or fluoride-containing substances employed in dental prophylaxis or treatment, bacterial activity along with their metabolic byproducts, and an acidic environment may induce degradation of the titanium oxide layer and initiate the corrosion process [17, 18]. In the oral cavity, Ti surfaces are coated with proteins, including albumin. Research has shown that the presence of albumin could potentially hinder titanium corrosion. It has been hypothesized that albumin adsorption onto titanium may mitigate fluoride-induced corrosion, or that the buffering capacity of albumin could elevate the pH in the proximity of the titanium material [13].
The main issue of the present study was to evaluate fluoride's impact on titanium corrosion. During the review of the scientific literature, an analysis of 6 publications was carried out [8, 12-16]. In all studies, procedures were conducted in vitro using different fluoride concentrations on titanium (cpTi and Ti-6Al-4V) plates. Five studies were conducted on cpTi and two of them – were on Ti-6Al-4V alloy.
Furiya-Sato et al. [15] underscored that immersing commercially pure titanium (cpTi) in a 1000 ppmF NaF solution at pH 6.5 did not elicit any discernible changes in the electrochemical corrosive characteristics of the titanium samples. However, immersion in a 9000 ppmF NaF solution at pH 5.3 led to considerable corrosion. It is recognized that hydrogen fluoride (HF) can trigger titanium corrosion by disrupting the surface oxide layer. HF can be produced from fluorine ions in acidic environments. So because of neutral pH, 1000 ppm NaF didn’t cause corrosion [15]. However, it should be noted that a lower concentration of fluoride can still cause corrosion on the surface of titanium if acidification occurs due to eating and drinking. The presence of biofilm on the titanium surface contributes to the creation of an acidic environment through the metabolism of sugar. Fukushima et al. [12] confirmed that the presence of Streptococcus mutans cells on the titanium surface adversely affected the corrosion resistance of titanium. Conversely, significant corrosion was induced by 9000 ppmF NaF through the efficient formation of hydrogen fluoride (HF) due to its elevated fluoride concentration and acidic pH [15].
A study by Shuto et al. [19] that evaluated changes to titanium surface based on the fluorides and abrasives in toothpaste pointed out that the biggest value changes in surface roughness, alterations in titanium color and gloss was brushing pure-titanium discs with (fluoride+/abrasive+), then - (fluoride– /abrasive+) toothpaste slurry. It showed that the presence of fluorides impacted the titanium surface texture.
Goutam et al. [20] highlighted that the corrosion potential (Ecorr/V) of titanium implants in artificial saliva was measured at -0.42, whereas in artificial saliva containing 0.25% NaF, it was recorded as -0.63. Similarly, for Ti-6Al-4V, the Ecorr/V in artificial saliva was -0.56, while in artificial saliva with 0.25% NaF, it was -0.60. These differences were found to be statistically significant (p<0.05). Thus, the presence of fluoride exhibited a notable influence on the corrosion behavior of titanium implants.
The study conducted by Chen et al. [21] employs polarization analysis to elucidate that, in fluoride-containing oral environments with a neutral pH, the Ti-6Al-4V alloy displays inert characteristics. However, the alloy's vulnerability to acute corrosion becomes apparent in the presence of crevices. This corrosion is primarily attributed to localized acidification and the subsequent formation of HFO, which arises from the complexation of hydrogen ions (H+) and fluoride ions (F−).
Previous systematic reviews have demonstrated that fluoride can diminish the corrosion resistance of metallic implants. This occurs as fluoride ions within the electrolytic environment of the oral cavity precipitate onto the titanium oxide layer, thereby facilitating its dissolution [3, 18, 22-25].
70% of implant-supported restoration failures occur due to inflammatory reactions [22]. Contemporary dental practitioners encounter the challenge of managing peri-implant mucositis, which, if left untreated, may advance to peri-implantitis, leading to marginal bone resorption and ultimately implant failure [17, 22].
Systematic reviews elucidating findings from in vitro experiments have underscored the propensity of titanium ions or particles to evoke toxicological or pro-inflammatory responses [3, 17, 18, 22-26]. Titanium particles that are shed from the implant surface are immunogenic. When titanium corrodes, particles are released from Ti-based implants and can be found in the tissues and organs surrounding the implants. In addition, discoloration and changes in gloss and surface roughness may also be observed [27]. Research studies have identified titanium as the predominant foreign body found in biopsies of peri-implantitis, with these metal particles being surrounded by inflammatory cells within the tissues. Macrophages ingest titanium particles and produce pro-inflammatory cytokines, which are associated with the activation of osteoclasts. Nanoparticles of metal oxides, particularly TiO2, exhibit antimicrobial properties. There is a suggestion that titanium debris could disrupt the delicate equilibrium between bone formation and resorption, subsequently precipitating osteolysis and bone resorption [18, 23-25]. Through this mechanism, titanium ions could plausibly participate in inflammatory cascades, thereby contributing to the observed bone loss associated with peri-implant mucositis and peri-implantitis.
Moreover, an upsurge in titanium ion concentration within afflicted sites may arise from corrosion instigated by the activity of inflammatory cells and bacteria residing in peri-implantitis lesions, consequently leading to a reduction in pH levels within the peri-implant milieu. The accretion of bacteria and oral biofilm contributes to oral pH reduction, thereby fostering titanium corrosion, even at relatively lower fluoride concentrations. The results indicate that inflammation disrupts both the functional properties and structural composition of biofilm, leading to corrosion [23, 24].
Conclusion
Pure titanium and titanium alloys are susceptible to corrosion in acidic environments, even at low fluoride concentrations. Both acid and fluoride play crucial roles in initiating titanium corrosion, as decreasing pH levels necessitate lesser fluoride concentrations to trigger corrosion development. These observations highlight the potential for fluoride exposure to induce corrosion of dental implants, thereby contributing to the onset of mucositis and peri-implantitis processes.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None