COMPARATIVE STUDY: PHYSICAL AND CHEMICAL PROPERTIES OF NEW “CERAFILL” VERSUS OLD “IROOT” BIOCERMIC ROOT CANAL SEALERS
Abeer Abdulaziz Mokeem Saleh1*
1Department of Endodontic, Faculty of Dentistry, King Abdulaziz University, Jeddah 22252, Saudi Arabia. [email protected]
https://doi.org/10.51847/8mcX7DGVK3
ABSTRACT
The new Bioceramic “Cerafill” root canal sealer launched in the market with a lack of the knowledge about its physical properties. This study aimed to evaluate its properties as compared with the old version “iRoot”. The fresh past of each sealer was subjected to setting time test. The set discs were immersed in deionized water to determine solubility%, pH changes, calcium ions (Ca++) released after 1, 7, 14 and 28 days. The flowabilty and film thickness of each sealer was also determined. The ANOVA statistical test was used at P < 0.05. Cerafill showed the significant faster setting time (initial and final) and significant lowest solubility% than iRoot (P<0.001). Both Cerafill and iRoot exhibited high alkaline media ranged (9.17-11.52) and released Ca++ (P<001), with no significant difference between them. The greatest flow and lowest film thickness exhibited by iRoot (22.2 ± 0.12 mm and 50 ± 0.2 µm respectively) versus Cerafill (19.5 ± 0.5 mm and 70 ± 20 µm respectively). The new Cerafill has better physical properties regarding setting times, solubility, pH changes, Ca++ releasing, flowability and film thickness that meet the requirements for ideal root canal sealer.
Key words: Root canal sealers, Bioceamic root canal sealers, Physical properties, iRoot, Cerafill.
Introduction
For effective endodontic therapy, the sealer is required to fill the irregularities and spaces within the obturating material. Various types of sealer were used to create a fluid-tight seal and prevent microleakage within the obturation [1]. Bioceramic-based sealer is one of these sealers and has been available since 2009 [2]. It is mainly composed of calcium silicate and calcium phosphate, which promotes bioactivity and produces chemical apatite when exposed to tissue fluid present within the dentinal tubules, consequently providing a tight sealing [3]. The injectable premixed paste version of several brands of bioceramic root canal sealers is offered, including iRoot (BC, Innovative BioCeramix Inc, Vancouver, Canada). In an earlier study, the physical and chemical properties were evaluated [4]. Its solubility finding was higher than the acceptable limit (3%) [4-6].
Recently, a new bioceramic-root canal sealer “Cerafill” (Prevest DenPro, Jammu, India) has been developed. Based on manufacturer guidelines, it is a premixed calcium silicate sealer containing aluminum-free, calcium phosphate, bioactive glass particles, and zirconium oxide (as a radio-opacifier) [7]. It claimed to be having excellent physical properties. The articles demonstrating their physiochemical behavior are currently insufficient.
This study aimed to compare the physical and chemical properties of Cerafill versus iRoot bioceramic including; setting times, solubility %, pH changes, released calcium ions, flow, and film thickness. According to the null hypothesis, there was no difference between the three investigated sealers used in this study
Materials and Methods
The procedures of this study were started after agreement from the ethics committee of King Abdulaziz University. Two calcium silicate Bioceramic-based root canal sealers; Cerafill and iRoot were evaluated. AHplus; (Epoxy resin, Dentsply, De Trey, Germany) was used as a gold standard control sealer.
Setting time
For each sealer, ten samples (n=10) were prepared according to the manufacturer's instructions based on ISO 6876/2012 [8]. In a 10 mm internal diameter and 2 mm height mold, the injectable paste of bioceramic sealers and a fresh mixture of AH-Plus were placed. Every 15 minutes, beginning after 30 minutes, a Vicat needle (Jin-Ching-Her, Taiwan), having 50 mm length, 10 mm diameter, and 100 g weight, was periodically inserted, on the sample surface When the needle was difficult to penetrate within the sealer, it indicates the time of initial setting. However, when no visible depression was detected on the surface of the sealer, it indicates the time of complete sets [9].
Solubility %
The initial weight (W0) of each disc (n=10) was performed by an electric balance (Scientech, USA); after it had fully hardened. It was then put in a tube containing deionized water (10mL). All samples were incubated at 37 °C/100% humidity. All discs were taken out after each experimental period (1, 7, 14, and 28 days), allowed to dry overnight, and then weighed again (Wt1, Wt7, Wt14, and Wt28). The following Equation [10] was used to calculate the solubility percentage (%).
|
|
(1) |
pH changes
The pH of the solution at 1, 7, 14, and 28 days was assessed using the pH meter (Bibby Scientific, UK). The pH meter was previously calibrated using reference solutions of 4.0 & 7.0 pH [4].
Calcium release
The solution of each solubility period (1-28 days) was evaluated using the EDTA titration technique to determine the releasing calcium ions (Ca++) [11, 12].
Sealer flow and film thickness
The flowability test was carried out based on ISO 6876/2012 for root canal sealers, (8,12). Five samples of each sealer were prepared. On a glass slab (n=5) measuring 35 by 35 by 6 mm3, one drop of 0.05 volume was placed. After three minutes, a second glass slab of 20 mg and an additional 100 g weight was added to the top of the spreading sealer. At 37 degrees Celsius and 100% humidity incubator, the sealer within the glass slabs and 100 g weight were placed for 10 minutes. Using a digital caliper (Cole-Parmer, Montreal, Canada), the dimensions of the circular sample were measured after the upper glass slab and top weight were removed. The test was repeated if the resulting circle had an uneven diameter or if it was larger than 1 mm [10].
Following the flowability test, the thickness of both glass slabs containing the sealer (Ts) was measured by a digital caliper. An empty double slab thickness (T0) was also determined. The equation (Ts-T0) was used to calculate the film thickness of each sealer [8, 10].
Statistical analysis
All the recorded data; including setting time, solubility%, pH variations, Calcium ions released, sealer flow, and film thickness were statistically analyzed at a significance level of 5% using SPSS software (Version 16.0; Chicago, IL) to compare the investigating sealers. According to Shapiro-Wilk (>0.05), One-way ANOVA and Tukey tests were used.
Results and Discussion
Setting time
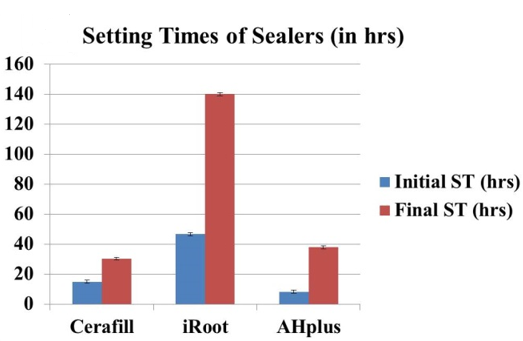
Figure 1a illustrates the mean ± standard deviation (SD) of the setting times (initial and final) recorded by the three root canal sealers. AHplus exhibited the significant fastest setting times initial as well as final times, however, the significant delayed setting times (initial and final times) were detected by iRoot (P < 0.001).
Solubility %
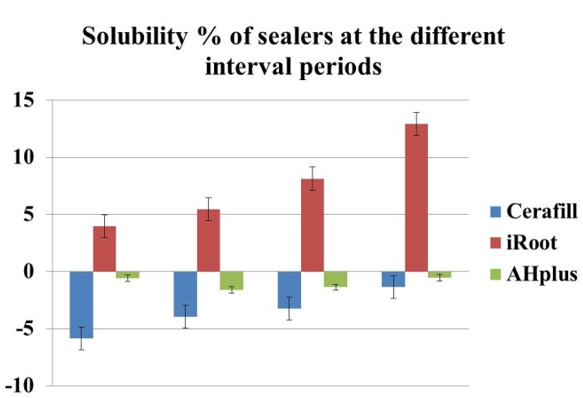
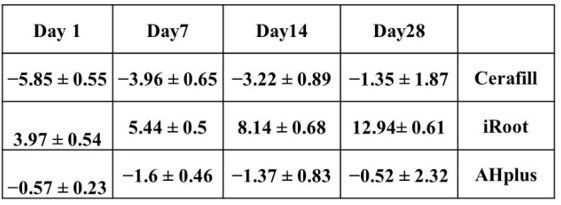
Figure 1b illustrates the mean ± SD values of the solubility% of the investigated root canal sealers among the experimental periods. iRoot sealer exhibited a significantly greater solubility% at all immersion times (from the first day up to 28 days. However, Cerfill and AHplus were determined to gain weight with the significantly greatest values exhibited by Cerafill sealer (P < 0.001).
|
|
|
a) |
|
|
|
b) |
|
Figure 1. The mean ± SD of setting times (a) and solubility% (b) of the investigated sealers among the experimental periods. |
pH Change
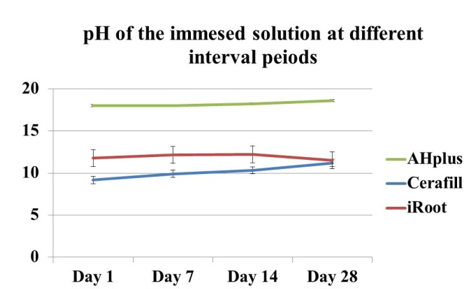
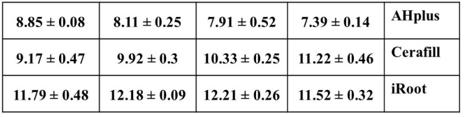
Figure 2a illustrates the mean ± SD values of pH changes of the sealers during the experimental periods. On day 1, the storage deionized water of AHplus showed weak alkaline (8.85 ± 0.08) that decreased gradually to be nearly neutral (7.39 ± 0.14) on day 28. However, both Cerafill and iRoot sealers exhibited high alkaline solutions (ranging between 9.17 -11.52) among all experimental periods. The significant greatest values were obtained by Cerafill (P < 0.001), with no significant difference between Cerafill and iRoot at day 28 (P= 0.137).
Calcium ions released
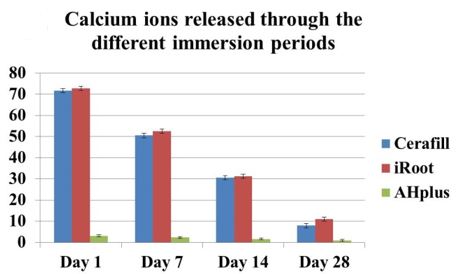
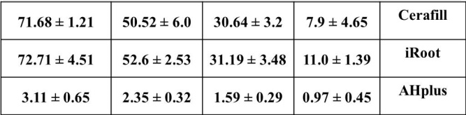
Figure 2b illustrates the mean ± SD values of the calcium ions released from all investigated root canal sealers among all the experimental periods. The iRoot sealer exhibited significantly greater mean values of the released material (P<0.001) at all experimental periods with no statistical significance between iRoot and Cerafill (P> 0.05). However, at all experimental times, AHplus detected a significantly low mean value (P< 0.001)
|
|
|
a) |
|
|
|
b) |
|
Figure 2. The mean ± standard deviation (SD) of pH changes (a) and calcium ion release (b) of the three sealers during the experimental period. |
Sealer flow and film thickness
The significant greatest mean flowability was recorded by iRoot (22.2 ± 0.12 mm), followed by AHpus (21.4 ± 0.41 mm), whereas the Cerafill determined the significant lowest mean value (19.5 ± 0.5 mm), at P < 0.001. Regarding the film thickness, Cerafill showed a significantly greater mean value (70 ± 20 µm, at P<0.001), however, both iRoot and AHplus provided nearly similar film thickness (means values 50 ± 0.2 and 51 ± 0.1 µm respectively). There was an insignificant difference between iRoot and AHplus (P> 0.05).
According to the proposed requirements of ideal root canal sealers suggested by Grossman and ADA specification #57 [13, 14], the physical and chemical properties of the sealers, affect the performance and quality of obturation [15]. In the current study, the physic-chemical properties including setting times, solubility, pH, Ca++ released, flow, and film thickness of recent “Cerafil” compared with old ”iRoot” bioceramic sealer. According to the current finding of bioceramic sealers, the results of setting times, solubility%, flow, and film thickness rejected the null hypothesis, while the pH and released Ca++ were accepting the null hypothesis.
Setting time should be an initial reasonable time permitting the suitable working time while it is finally set within a short time to possibly eliminate the periapical irritation [13, 16]. The Cerafill determined the significantly fastest initial as well as final setting times (14.89 ± 0.53 and 30.22 ± 0.19 hrs respectively) than that of iRoot (46.65 ± 1.85 and 140.1± 5.02 hrs respectively). In previous studies, all bioceramic sealers failed or take a too prolonged time to complete the set [17, 18]. The moistened environment is essential for the hydration reaction of the bioceramic sealers to promote the formation of the calcium silicate hydrate phase that is responsible for complete sealer hardening. In accordance, the same finding of prolonged setting time for iRoot was recorded by several studies [19, 20]. Loushine et al. stated that “The endosequence root canal sealer needs at least 7 days for a complete set, even in different environments of humidity [21]. The difference in results in both Bioceramic sealers may be attributed to the lack of sulfate phase in iRoot. However, the calcium phosphate contents of Cerafill “as described in the manufacture brochure” [7], are responsible for fast setting since it is considered a reactive phase and controls the calcium silicate material hydrates [22]. The control AHplus had a fast setting time starting from 8.3 ± 0.64 to 37.86 ± 1.52 hrs until the final set. Inconsistent, in a previous study [23], AHplus took 10- 12 hrs for setting a time [23, 24] that was attributed to its epoxy amine polymerization reaction [24].
The sealer’s solubility could affect the lifespan of endodontic prognosis. It could lead to the sealer degrading, jeopardizing the apical seal, and enhancing bacterial leakage [25, 26]. According to ISO 6876, the weight loss during the solubility test has not exceeded 3% [8]. In the current study, iRoot exhibited a significant great solubility% (ranging from 3.97-12.94 within the 28 days experimental periods) that goes beyond the acceptable limit. It may be attributed to its delay in the setting time that allows the degradation of its particles. However, Cerafill and AHplus have gained weight with significantly greater values obtained by Cerafill. Regarding AHplus, it was supported by a previous study that attributed to its ability to water sorption and great expansion during resin polymerization [25]. Up till now, there was no publication related to the physical properties of Cerafill. Its gain weight may be attributed to water diffusion within its polymerized particles due to its calcium sulfate phase [27].
The alkaline medium and releasing Ca++ are essential to neutralize the inflammatory condition and promote the healing of periapical tissue and enhance dentin mineralization. Both Cerafill and iRoot sealers exhibited high alkaline solutions and great Ca++ release among all experimental periods (Figure 2), with no significant difference between them (P > 0.05). All the previous studies determined high alkaline medium around bioceramic sealers [4, 6, 18, 20]. There was a relation between pH changes and releasing Ca++. The more alkaline pH, the greater Ca++ is released. It is attributed to the calcium hydroxide by-product that is produced during the setting reaction of calcium silicate [19]. When this calcium hydroxide, in turn, reacts with water, it dissociated into hydroxyl ions (OH− ) and Ca++. The hydroxyl ions (OH−) promotes the alkaline medium [28] that is favorable for antimicrobial activity [29, 30], while Ca++ enhances dentin mineralization and bioactivity when exposed to tissue fluid [3]. However, the control AHplus exhibited initial weak alkaline that decreased to neutral pH. It is indicative of the small amount of calcium hydroxide within its composition that decreased after resin polymerization. This finding was accepted by many studies [17, 28].
Flow and film thickness properties are essential for improving the dentin adaptation and sealing ability of root canal obturation and, in turn, preventing microleakage [29]. However, the excessive flow may provoke tissue irritation if the sealer extruded into periapical tissue [31]. The three investigated sealers had flow quality and film thickness acceptable by ISO standards 6876 [8], with greater flow value obtained by iRoot (22.2 ± 0.12 mm) and greater film thickness obtained by Cerafill (70 ± 20 µm). It may be attributed to its delayed setting times of iRoot and the fast setting of Cerafill. Similarly, previous studies determined a high flow of Bioceramic sealers (ranging between 23-26 mm) [20]. On the contrary, AHplus previously determined a higher flow (37.97 ± 0.55 mm) than that of calcium silicate MTA-Fillapex (29.04 ± 0.39 mm).
Conclusion
The new bioceramic “Cerafill sealer meets the ideal requirements of root canal sealer. It has superior setting time and eliminates solubility properties versus the old “iRoot” sealer. It promotes pH media and released Ca++ that may contribute to antimicrobial activity, biocompatibility, bioactivity, and periapical tissue healing potentiality. It also has acceptable flow and film thickness. It needs further investigation to assess its adaptation and sealability.
Acknowledgments: The author would like to thank the Advanced reseach lab in Faculty of Dentistry of King Abdulaziz university (KAUFD) as all laboratory tests were permitted.
Conflict of interest: None
Financial support: None
Ethics statement: The procdures of the current study was approved by Ehical committee of KAUFD.