Currently, extraction is increasingly avoided to alleviate crowding. This study aimed to evaluate changes in the buccal alveolar bone during the alignment phase of orthodontic treatment without extractions using cone beam computed tomographic. Two reviewers, without regard to language limitations, performed a manual search through June 2024 and an electronic search of web databases (Medline, Science Direct, Scopus, and Web of Science). Clinical studies, both randomised and non-randomized, were considered. Utilising the Cochrane risk of bias tool for randomised trials, the same reviewers evaluated the studies' quality. And the Methodological Index for Nonrandomized Studies (MINORS). A total of 2815 records were initially identified. Following title and abstract screening, the full texts of thirty studies were reviewed, and eight studies met the selection criteria and were included in the review. All studies reported unfavourable changes in the bone structure following non-extraction treatment, affecting both the bone thickness and height of maxillary and mandibular incisors; premolars, and the mesiobuccal root of maxillary first molars. Non-extraction alignment of dental crowding resulted in significant bone loss, of both bone thickness and height. These results must be taken into account in non-extraction treatments, to prevent the iatrogenic effects of this therapeutic approach.
Introduction
The aim of orthodontic treatment is not only to enhance dental aesthetics and function or to achieve optimal occlusion but also to maintain or improve the health of periodontal tissues [1]. In non-extraction treatment, especially in crowded cases, it is necessary to create space in the dental arches. Without the extraction of permanent teeth; interproximal enamel reduction or distal movement of teeth, an increase in arch perimeter typically requires both transverse expansion and proclination [2, 3]. Dental arch expansion and buccal-lingual movements of teeth can move teeth beyond their bone envelope, potentially causing dehiscence, fenestration, and gingival recession, depending on the initial morphology of alveolar bone and the amount of tooth movement [4].
Expansion of dental arches utilizing self-ligating brackets and broader super elastic arch wires has become an issue [5, 6]. Different passive and active self-ligating brackets have been introduced with claims of reduced friction, light forces, efficient sliding mechanics, and easy clinical application [7, 8]. Damon System®, for example, claims it is possible to achieve large gains in arch perimeter and transverse dimension without the use of rapid maxillary expansion. This system can expand arches and create or move the supporting tissues, decreasing the need for extractions and increasing overall stability [9]. Nevertheless, many of these findings remain controversial.
Before the introduction of computerized tomography, it was not possible to visualize the buccal bone due to superposition that occurred in 2D radiographs. The advent of cone-beam computed tomography (CBCT) has allowed for more extensive studies evaluating alveolar bone. CBCT is indeed a valuable tool for quantitatively assessing the height and thickness of the buccal bone with high precision and accuracy [10-12].
The purpose of this study was to assess changes in the buccal alveolar bone during the alignment phase of orthodontic treatment without extractions. This assessment is crucial to prevent iatrogenic effects on the sustaining and protection periodontium, such as gingival recessions, dehiscence, and bone fenestrations.
Materials and Methods
Protocol and registration
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis were followed in this work, which was registered in the PROSPERO database with the identifier CRD42024554659 [13-15].
Eligibility criteria
This systematic review included studies that met predetermined eligibility criteria, with inclusion and exclusion parameters established according to the PICOS framework.
The exclusion criteria were:
Information sources and search strategy
Electronic searches were carried out in the following databases: PubMed, Science Direct, Scopus, Web of Science, and EBSCO, by two reviewers, combined with a manual search, without time and language restriction, up to June 2024. The search strategy used several MeSH and free terms joined by Boolean operators: "Compact computed tomography" OR "CBCT" AND "arch expansion" AND "Alveolar bone" OR "Alveolar bone thickness" OR "bone height" AND conventional brackets AND self-ligating brackets.
Study selection and data extraction
In order to determine the studies' eligibility according to the inclusion criteria, two independent writers (CM and OH) first looked over the titles and abstracts. After this preliminary screening, the entire texts of the publications that seemed qualified for the review were assessed. Disagreements were settled by consulting a third author (BH). The review rejected studies that failed to meet one or more inclusion criteria.
Risk of bias assessment
Two authors (MC and BE) assessed the quality of the selected studies using Cochrane's risk of bias tool for randomized clinical trials (RoB 2.0). The RoB 2.0 assessment tool is organized into five different domains: randomization process, deviation from intended intervention, missing outcome data, measurement of outcome, and selection of reported result. Each domain was assessed using one of the following options: low risk, some concern, or high risk. Any disagreements between the two authors were resolved through discussion with a third author (BH).
The Methodological Index for Nonrandomized Studies (MINORS) was utilized to assess the methodological quality of non-randomized clinical studies, this tool was specifically designed and validated for evaluating both comparative and non-comparative nonrandomized studies. For non-comparative studies, only the first 8 of the 12 MINORS criteria were assessed. Each item on the scale was scored as 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate), with the maximum ideal score being 16. For comparative studies, all 12 MINORS criteria were assessed, with the maximum ideal score being 24. Any disagreements were resolved through discussion with a third author (BH).
Results and Discussion
Study selection
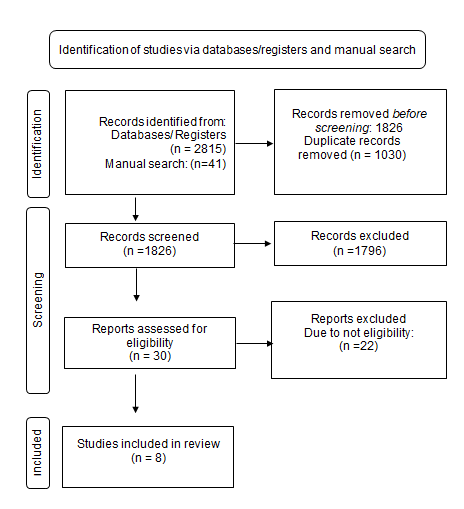
The electronic database search identified a total of 2815 items, with an additional 41 articles identified through manual search. After removing duplicates, 1826 articles remained. Following a screening of titles and abstracts, 1796 articles were excluded. Thirty articles were selected for full-text review. Of these, eight articles (11.12.13.14.15.16.17.18) were deemed eligible and included in the final systematic review (Figure 1).
|
|
|
Figure 1. Prisma 2020 Flow Diagram of Article Selection for Systematic Review |
Study characteristics
The characteristics of the included studies are summarized in (Table 1). Among the eight selected studies, three are prospective studies, three are retrospective studies, and two are randomized controlled trials (RCT). All selected articles examined alveolar bone changes using CBCT following treatment without extractions or stripping. Most studies included both male and female participants, though some studies did not specify the gender. The mean age of patients across all studies ranged from 14.7 to 22.3 years. None of the studies reported a long follow-up period. A total of 214 patients were included in the studies. Each patient underwent CBCT examinations before (T0) and after treatment, with observation periods varying between 6 months and 2.83 years.
In the selected studies, various types of orthodontic treatments were evaluated and compared, including self-ligating vs. conventional brackets. They also evaluated passive self-ligating appliances and compared passive and active self-ligating brackets. All CBCT images were at high resolution with different exposure parameters and with a reported voxel size ranging from 0.08 mm to 0.4mm.
Table 1. Study characteristics
|
Age |
Sex |
Simple size |
Study design |
|
|
mean age 19.55 |
11 male 10 female |
21 patients |
retrospective |
Calil et al. 2020 |
|
Passive (SLB) group: 16.0 ±5.7 years active (SLB) group: 15.0± 3.3 years |
Not reported |
41 patients |
RCT |
Cattaneo et al. 2011 |
|
mean age 22.3 years |
10 female 6 male |
16 patients |
prospective |
Ibiapina et al. 2016 |
|
passive (SLB) group 18.58 ±5.43 years (CB) group 21.61 ±6.69 years |
Not reported |
25 patients |
RCT |
Almeida et al. 2014 |
|
the mean age of 14.7 years |
9 Female 13 male |
22 patients |
prospective |
Morais et al. 2018 |
|
mean age 14.9 ±1.16 years |
10 males 2 females |
12 patients |
Retrospective |
Pinzan-Vercelino et al. 2023 |
|
the mean age of 14.7 years |
9 Female 11 male |
20 patients |
prospective |
Abdelshaf et al. 2021 |
|
mean age 18.7 ± 10.8 years |
17 males 40 female |
57 patients |
Retrospective |
Garlock et al. 2016 |
Risk of bias in individual studies
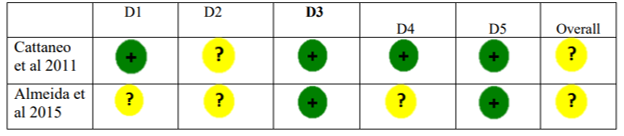
Among the two [16-18] clinical trials, only one [16] adequately reported the method of randomization and described the blinding of examiners during treatment procedures. Neither trial provided an adequate description of allocation concealment. Blinding of participants was not mentioned in any of the studies. Both trials documented the number of patients at baseline and final examination. Furthermore, only one trial reported a sample size calculation [17]. The two studies were considered to have an unclear risk of bias Figure 2. Regarding the non-randomized studies, MINORS scores ranged from 8 to 15 out of a possible 16 for non-comparative studies [19-21] and from 17 to 22 out of a possible 24 for comparative studies [22-24]. Several limitations were identified, including the absence of consecutive inclusion or unclear reporting of consecutive inclusion (item 2), and the retrospective nature of data collection (Table 2).
|
|
|
Figure 2. Risk of bias assessment of RCTs using the ROB-2 tool. The different domains have been defined by D1 to D5 (D 1: Randomization process; D 2: Deviations from the intended intervention; D 3: Missing outcome data; D 4: Measurement of the outcome; D5: Selection of the reported result) |
Table 2. Methodological index for non-randomized studies (MINORS)
|
Minors score |
||||||||||||||
|
Authors |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
Total |
|
|
Morais et al. 2018 |
2 |
1 |
1 |
2 |
2 |
2 |
1 |
2 |
|
|
|
|
13 |
|
|
Garlock et al. 2016 |
2 |
0 |
0 |
2 |
2 |
2 |
0 |
0 |
|
|
|
|
8 |
|
|
Pinzan-Vercelino et al. 2023 |
2 |
1 |
2 |
2 |
2 |
2 |
2 |
2 |
|
|
|
|
15 |
|
|
delshaf et al. 2021 |
2 |
1 |
2 |
2 |
2 |
2 |
2 |
2 |
2 |
2 |
1 |
2 |
22 |
|
|
Ibiapina et al. 2016 |
2 |
1 |
2 |
2 |
2 |
2 |
2 |
0 |
2 |
2 |
2 |
2 |
21 |
|
|
Calil et al. |
2 |
1 |
0 |
2 |
2 |
2 |
2 |
2 |
|
1 |
1 |
2 |
17 |
|
Results of individual studies
All studies reported unfavourable changes in the bone structure following non-extraction treatment. In all articles comparing two types of appliances, no significant differences were observed between the groups. Four studies utilized passive self-ligating brackets [19-22], one study [16] used both passive and active self-ligating appliances, and three studies [17, 23, 24] compared passive self-ligating appliances with conventional brackets (Table 3).
Table 3. Results of individual studies
|
Alveolar bone changes |
transverse changes |
Teeth |
CBCT settings |
Observation Period |
Type of Appliance |
|
|
Buccal bone thickness (BBT)mm: 1 mb:-0.41 1 dm:-0.39 2PM:-0.10 p=0.000 1 PM: -0.55 p=0.024 C:-0.70 p=0.00 |
3-3 (mm): +1.44 4-4 (mm): +3.16 5-5 (mm): +2.90 6-6 (mm): +2.44 |
1M 1PM 2PM C |
7 mA, 85 kV, E.T: 14.4 s, V.S: 0.08 mm |
T0 = before treatment T1 = after 6 months |
passive Self- ligating brackets (SLB) |
Calil et al. 2020 |
|
Buccal bone thickness active (SLB): 18-23% Passive (SLB): 12-17% bone area (BA) mm2: active (SLB): - 3.6 ± 3.6 mm2 Passive (SLB): -2.3 ± 3.5 mm2 |
Reported on the digital models |
1 PM
|
0.36-mm isotropic voxel |
T0 = before treatment T1 = after 22.4 months for passive (SLB) and 21.1 for active (SLB) |
passive (SLB) group: n=21 active (SLB) group:n=20 |
Cattaneo et al. 2011 |
|
Buccal bone thickness for GI / GII respectively: C –0.067/ -0.069 1 PM –0.03/- 0.16 2 PM –0.06/- 0.20 M –0.11/- 0.02 |
Reported on the dental casts using a digital caliper |
1M 1 PM 2 PM C |
36 mA, 120 kV, E.T: 40s, V.S: 0.4 mm |
T0 = before treatment T1 = after 6 months |
conventional group: n=8 passive(SLB) group n=8 |
Ibiapina et al. 2016 |
|
Buccal bone thickness: CB group: 1 PM -1.51 mm, p = 0.016 2 PM-1.09 mm, p = 0.007 M -0.79 mm, p = 0.008 SLB group : 1 PM -0.88 mm, p = 0.019 2 PM -1.09 mm, p < 0.001 M -0.54 mm, p=0.025 |
Reported on the dental casts using a digital caliper |
1LM 1LPM 2LPM |
36 mA 120 kV, E.T: 40s, V.S: 0.4 mm |
T1 = before treatment T2= 7 months after treatment onset |
passive (SLB) group: n=13 conventional group: n=12 |
Almeida et al. 2015 |
|
Buccal bone thickness : 1 I -0.2 p=0.000 2 PM-0.2 1M mb - 0.6 p=0.000 Bone height (BH): 1 I -0.4mm p=0.000 2 PM-0.1 1M mb - 0.3 Bone area (BA) mm2 : 1 I -1.2 p=0.000 2 PM-0.4 1M mb – 4.3 p=0.000 |
1PMs +4.3 mm p=0.000 1Ms + 2.3 mm p=0.000 |
1 I 2 PM 1M |
5 mA, 120 kV E.T: 20/40s, V.S: 0.3/0.25 mm |
T0 = before treatment T1 = 53.6 weeks |
passive self-ligating brackets |
Morais et al 2018 |
|
Bone height: 1U -0.74 p=0.000 2U -0.85 p=0.000 1L -0.88 p=0.000 2L - 0.86 p=0.001 |
Not reported |
1I 2I 1i 2i |
5 mA, 120 kV E.T: 20s, V.S: 0.3 mm |
T1= before treatment T2 =2.83 years |
passive self-ligating brackets |
Pinzan-Vercelino et al. 2023 |
|
Buccal bone thickness for 1I ; 2PM and mb1 respectively: (GI) : 1.3/2.5/1.36 (GII) : 1.3/2.6/1.41 Bone height for 1I ; 2PM and mb1 respectively: respectively: (GI) : 1.7/0.7/1.4 (GII): 1.8/0.8/1.3 |
the results are unclear missing data |
1I 2 PM mb1, |
5 mA, 120 kV E.T: 20/40s, V.S: 0.3 mm |
T1= before treatment T2 =13.5 weeks (GI) T2 =15.5 weeks (GII) |
conventional group: n=10 passive(SLB) group n=10 conventional brackets group I (GI) and passive self-ligating group II (GII) |
Abdelshaf et al. 2021 |
|
Buccal bone thickness 1i MFCB:0.10 p=0.05 1i MLCB 0.29 p<0.01 Bone height 1i :1.12 mm p<0.01 |
Not reported |
1i |
5 mA, 120 kV E.T: 4.8s V.S: 0.3 mm |
T1= before treatment T2= 22.7 ± 7.3 months |
passive self-ligating brackets |
Garlock et al. 2016 |
Changes in the maxillary teeth
Regarding maxillary incisors, three studies [19, 20, 24, 25] assessed alveolar bone changes, reporting reductions in buccal bone thickness (BBT) ranging from -0.2 mm to -1.3 mm, and decreases in bone height (BH) ranging from -0.4 mm to -1.8 mm. For maxillary canine, two studies [22, 23] examined buccal bone thickness, revealing reductions between -0.067 mm and -0.70 mm. Five studies [16, 19, 22-24] evaluated alveolar bone changes in maxillary premolars, the buccal bone thickness (BBT) values ranged between (-0.2; -2.5mm), and bone height (BH) between (-0.1; -0.8mm). Concerning maxillary mb1 [19, 22-24] 11.13.15.17 (BBT) values ranged between (-0.41; -1.4mm), while bone height (BH) reductions ranged from -0.3 m to -1.4 mm. Studies [19, 22] assessing transverse changes consistently indicate that expansion predominantly affects the first premolar.
Changes in the mandibular teeth
Two studies [20, 21] evaluated bone height (BH) in the lower anterior teeth, reporting an average buccal vertical bone loss ranging from -1.12 mm to -0.88 mm. Another study [17] assessed buccal bone thickness (BBT) in premolars (PM) and molars, revealing decreases of -1.5 mm and -0.79 mm, respectively.
The main purpose of this study was to evaluate the effects on the buccal alveolar bone when using brackets and arch wire expansion to alleviate crowding without resorting to tooth extraction. Treatment philosophies in the 21st century tend to preserve dental tissues and try to limit extractions as much as possible. Especially with the introduction of self-ligating brackets which are supposed to provide a significant reduction in friction and when a light arch wire is used, while alignment occurs, the arch wire slides posteriorly, thus this approach avoids excessive anterior movement of the incisor teeth and obtaining spaces mainly through an lateral dentoalveolar expansion, known as “posterior transverse adaptation” [26, 27]. However, the alignment and levelling of dental crowding without extraction involve an increase in arch perimeter, achieved through incisor advancement and transverse expansion, as described for both conventional brackets (CB) and self-ligating brackets (SLB) [28].
Before the introduction of CBCT, it was impossible to measure the buccal or palatal bone plates accurately. Currently, alveolar bone height and thickness measurements can be achieved from CBCT images with good to excellent repeatability. However, the accuracy of alveolar bone height and thickness measurements depends on the voxel size [29]. When alveolar bone thickness is greater than CBCT voxel size (0.4 mm), alveolar bone height measurements are likely to be overestimated by 0.5 to 1 mm. When alveolar bone thickness is near or smaller than CBCT voxel size (0.4 mm), alveolar bone height measurements are likely to be underestimated by 0.9 to 1.2 mm. Decreasing CBCT voxel size from 0.4 to 0.25 mm can improve the accuracy of alveolar bone linear measurement from the CBCT images [30].
According to the findings of this systematic review, alleviating dental crowding without extraction leads to a reduction in both alveolar bone thickness and marginal bone level. Significant marginal bone loss was observed in all mandibular and maxillary incisors. Garlock et al. [21] reported an average buccal vertical bone loss of 1.12 mm in the mandibular central incisors, while Pinzan-Vercelino et al. [20] documented a 0.88 mm loss in the lower central incisors. Morris et al. [19] observed a significant decrease in bone thickness (BT) at the maxillary incisors, with a reduction of 24% in BT and a 13% decrease in bone area. Similarly, Abdelshaf et al. [24]. found a 1.8 mm decrease in BT at the upper incisors. Steiner et al. [31] using an experimental model, showed that 3.05 mm of labial incisor movement caused an average of 5.48 mm of vertical bone loss. It also appears that when the vertical bone recession does occur, the thickness of the cortical bone changes. It was observed that on the surface where vertical bone recession happened, thinning of the cortical bone on the same side also occurred, whereas the opposite side showed less cortical bone thinning [21].
Despite Figueiredo et al. [32] reporting that the canines and first premolars were the teeth most affected by buccal bone dehiscence before arch expansion. Ibiapina et al. [23] reported that the reduction in bone thickness at the premolars (PM) was not significant. This contrasts with the findings of Cattaneo [16], who observed a 12–23% reduction in buccal bone thickness at the second premolars (2 PM), and Almeida et al. [17], who reported a 1.5 mm reduction in bone thickness. The divergence in these findings may be attributed to several factors, including the large variation in initial bone thickness, the smaller amount of expansion, the shorter treatment duration, and different methods of measurement [19].
Calil et al. [22] compared treatment outcomes between self-ligating appliances and miniscrew-assisted rapid maxillary expansion (MARPE). They concluded that there was a significantly greater reduction in buccal bone thickness at the canines and premolars in the self-ligating group compared to the MARPE group. The study also found a correlation between bone loss, initial crowding, and the amount of expansion in the premolar region. Since the MARPE device did not use premolar or canine anchorage, there was minimal buccal bone loss in these teeth.
Morris et al. [19] confirmed that patients with severe initial crowding and thin bone experienced a greater reduction in bone thickness (BT) in the second premolar (2 PM) region. This is because premolars undergo the most significant transverse expansion, which is often not true expansion but rather buccal tipping, it is known that buccal inclination may induce bone dehiscence and gingival recessions leading to greater buccal bone loss in this area [22].
The mesial roots of the maxillary molars may be at a higher risk of dehiscence compared to the distal roots due to thinner bone at the coronal level. Additionally, the mesial root is bulkier than the distobuccal root, rendering it more susceptible to dentoskeletal changes [29, 33]. Abdelshaf et al. reported a decrease of 1.4 mm in both bone thickness (BT) and bone height (BH). Morais et al. [19] reported a reduction of 0.6 mm in BT and 4.3 mm² in the bone area at the mesiobuccal root of the first molars. Similarly, other expansion devices have been associated with significant reductions in buccal bone plate thickness. Garib et al. [34] reported a reduction of 0.6 to 0.9 mm in the buccal bone plate thickness of the banded supporting teeth (first premolars and permanent first molars) for both tooth-tissue-borne and tooth-borne expanders, after 3 months of expansion. Brunetto et al. [35] compared rapid maxillary expansion (RME) with slow maxillary expansion and observed reductions in both bone height and thickness in both groups. In the study conducted by Calil et al. [22], which compared self-ligating appliances and miniscrew-assisted rapid maxillary expansion (MARPE) both groups demonstrated comparable buccal bone loss at the mesiobuccal root of the first.
Conclusion
Non-extraction alignment of dental crowding resulted in significant bone loss, affecting both the thickness and height of maxillary and mandibular incisors; premolars, and the mesiobuccal root of maxillary first molars. These results must be taken into account in non-extraction treatments, to prevent the iatrogenic effects of this therapeutic approach.
Limitation
The results of this systematic review are based on a limited number of studies. The absence of high-quality studies was the main limitation of this systematic review. Most of the available data are limited to short-term and medium-term outcomes without control groups; it would be relevant to investigate the periodontal status over the long term. Another significant limitation is the heterogeneity across the included studies, which may compromise the generalizability of the findings: The patient populations included both growing and adult individuals. Growing patients have a greater ability for bone remodeling, whereas adult patients are more susceptible to vertical bone loss during orthodontic treatment. Measurement of bone thickness at different levels (cervical, middle, and apical); The voxel sizes used in CBCT imaging varied across studies, this variation could introduce methodological bias, affecting the accuracy and comparability of the results. Future studies are needed with more standardized protocols in terms of patient selection and imaging parameters while including long-term follow-up and control groups to better assess the effects of orthodontic treatment on alveolar bone health.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None