
Assessment of Fluoride Uptake by Tooth Enamel from Different Fluoride Dentifrices: A Systematic Review
Mohammad Abdul Baseer 1*, Hanin Aloufi 2, Raza Alshaikh Ahmad 2, Sarah Alabdulwahab 2, Zahra Bu Khader 2, Osamah Mohammed AlMugeiren 3
1 Department of Preventive Dental Sciences, College of Dentistry, Riyadh Elm University, Riyadh – 11681, Saudi Arabia.
2 Dental Intern, College of Dentistry, Riyadh Elm University, Riyadh – 11681, Saudi Arabia.
3 Chairman, Department of Preventive Dental Sciences, College of Dentistry, Riyadh Elm University, Riyadh – 11681, Saudi Arabia.
ABSTRACT
Aim: To review the factors influencing the Enamel Fluoride Uptake (EFU) from different fluoride dentifrices by considering studies published between 2005 and 2020.
Materials and Method: This review study was based on a systematic search of the literature on fluoride uptake by dental enamel from fluoride dentifrices. This study was carried out in March 2020 by considering all published experimental studies. Structured search in different sources of bibliographic information. Source of tertiary information (Cochrane central register of controlled trials), sources of secondary information (PubMed, Saudi Digital Library and google scholar), and sources of primary information (review of relevant in each of the item selected) used the following keywords: "enamel fluoride uptake" and "dentifrice" or "toothpaste.
Results: A total of 3572 studies were identified from database searches. Only 34 articles were eligible for full-text retrieval. Of these, 22 articles were excluded as they failed to meet the inclusion criteria.
Conclusion: This review highlights that the EFU from fluoridated dentifrices depends on several factors, including the range of F compounds, F concentration, and pH of dentifrice, usage of mouth rinse, length of brushing, dentifrice quantity, and other added ingredients of the dentifrices. However, further studies are required to assess the effects of some other active agents of the dentifrices on the EFU.
Key words: Dentifrices, enamel, fluoride, uptake, EFU.
Introduction
Dental caries is one of the significant public health problems globally. 1-3 Dental caries arises from interactions between the tooth structure, the microbial biofilm formed on the tooth surface, and sugars, in addition to salivary and genetic influences. The caries mechanism consists of quickly alternating demineralization and remineralization cycles and, if net demineralization occurs over sufficient time, there will be the formation of the carious lesions.4 Many methods were adopted worldwide to prevent and control dental caries such as topical fluoride application, water fluoridation, school oral health programs, proper diet and regular clinic visits, the use of fluoride rinses, fluoridated floss, and fluoride dentifrice.5
Dental caries can be arrested or reversed by the continuous delivery of fluoride ions to the tooth surface.6 Therefore, fluoride products play a significant role in caries prevention by minimizing caries incidence and development in multiple pathways.7 These include such as decreasing Streptococcus Mutans and Lactobacillus colony counts,8 decreased bacterial acid production, decreased enamel apatite solubility, and fluoridation of apatite crystal surfaces decreased dissolution rate,9 and increased remineralization.10
Since the operative treatment of caries care is considerably expensive, the fluoride has proved to be an efficient means of caries prevention.11 As reported in many studies, topical fluoride applications are more successful in caries prevention than systemic fluoride applications.12 Dentifrices are commonly accepted as the necessary form of providing topical fluoride for caries-preventive benefits in addition to tooth brushing with toothpaste.13 At the same time, it is essential to promote oral health also at other levels of prevention such as good oral hygiene, healthy nutrition, regular check-ups, being included in oral preventive programs.11
Different forms of carriers are used for fluoride ions in fluoridated toothpaste, the most popular of which are sodium fluoride, sodium monofluorophosphate, and amine fluoride. Fluoride bioavailability is very critical for the caries-preventive effect and relies on the solubility of fluoride-containing compounds contributing to fluoride adhesion to the tooth surface. In vitro experiments indicate that inorganic and organic fluorides in dentifrice systems induce substantially different fluoride absorption on the tooth surface and have various remineralization consequences.14 Besides, the dentifrice amount and length of toothbrushing have a significant effect on the absorption and remineralization of enamel fluoride.15
In an in-vitro analysis, Friberger (1975) reported that decreased dentifrice pH affected increased EFU.16 Study by Marinho et al found that the usage of fluoride-containing mouth rinses or calcium chloride in combination with fluoridated dentifrices impacts EFU.17, 18 Besides, adding several additives to dentifrices such as anti-calculus or 'cosmetic' agents and natural substances may not have any influence on the remineralization mechanism and the EFU. 19-21
Hence, this paper aims to review the factors influencing the EFU from different fluoride dentifrices by considering studies published between 2005 and 2020.
Material and Methods
This review was based on a systematic search of the literature on fluoride uptake by dental enamel from different fluoride dentifrices. This study was carried out in March 2020 by considering all published experimental studies. The study proposal submitted to the Research Center of Riyadh Elm University, Riyadh, Saudi Arabia, and Institutional Review Board approval was obtained (FUGRP/2020/161/125/129).
Information sources
A structured search in different sources of bibliographic information was carried out by searching for keywords. Sources of tertiary information (Cochrane central register of controlled trials), secondary information (PubMed, Saudi Digital Library and google scholar), and primary information (review of relevant in each of the item selected) were searched by the following keywords: "enamel fluoride uptake" and "dentifrice" or "toothpaste." Preferred Reporting Item for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were utilized while performing the review.
Selection criteria
Inclusion criteria consisted of English publications on experimental studies involving permanent human teeth in which enamel fluoride uptake from fluoridated dentifrices was reported. The studies published in the last fifteen years (2005-2020) were considered for the review. While studies reported other than the English language, enamel fluoride uptake studies in primary teeth and bovine teeth were excluded from the review.
Screening
Step 1: Titles were reviewed by the authors and selected for further review for the abstracts if they met the inclusion criteria.
Step 2: Abstracts were reviewed and selected according to the same inclusion criteria used in step 1.
Step 3: Full-text articles of abstracts selected in step 2 were reviewed.
Step 4: The reference lists of all articles selected in step 3 were reviewed, and the full texts of potentially interesting studies were examined.
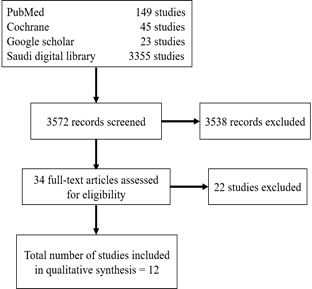
Fig. 1 Flow diagram of a systematic review of the literature.
Data extraction was performed by the investigators using a standardized form. The data extraction form included information on authors, year of the study, fluoride uptake measuring method, sample size, and concentration of fluoride, the quantity of dentifrice, duration (time), rinse used, and addition of cosmetic or active compounds, as shown in detail in Table 1.
|
Authors |
Year |
Aim |
Sample size |
Variables |
Findings |
|
Úbeda, Cardoso, and Buzalaf22 |
2005 |
Evaluate the F after using F dentifrice, preceded or not by a rinse with a CaCl2 solution |
10 participants |
Dentifrice: 1.5g NaF (1,000ppm F) Mouth rinse: 10mL of 20mM CaCl2 |
Pre-rinse with CaCl2 solution was not able to increase EFU |
|
Arnold et al. 14 |
2006 |
Investigate the effect of four different kinds of toothpaste with differing fluoride compounds on enamel remineralization |
90 extracted premolars (15 each group) |
Remineralization solution Dentifrices: Placebo, Elmex Anticaries(AmF), Elmex Sensitive (AmF), Blend-a-med Complete (NaF), Colgate GRF (NaMFP) |
EFU in an increasing order was NaF < NaMFP < AmF |
|
Nobre-dos-Santos, Rodrigues, Del-Bel-Cury, and Cury23 |
2007 |
Evaluate the enamel remineralizing ability of a formulation dentifrice with a low F concentration and low pH. |
6 participants wore removable appliance containing 6 enamel slabs |
Dentifrices- pH: 1, 100 μg F/g- pH 7.0 (positive control) 550 μg F/g- pH 5.5 (experimental) |
No significant difference was observed in terms of FBF, while LBF increased when the F concentration of dentifrice increased. |
|
Hattab24 |
2013 |
Assess the efficacy of different F dentifrices
Evaluate the effects of dentifrices on increasing EFU |
9 extracted premolars (cut into 36 sections) |
Dentifrices: 0.8% MFP-silica; 0.8% MFP-calcium carbonate and calcium phosphate; 0.8% MFP-calcium carbonate and calcium phosphate; 0.76% MFP-aluminium hydroxide; 0.24% NaF-silica and sodium pyrophosphate; 0.24% NaF-silica and sodium pyrophosphate; 0.76% MFP and 0.10% NaF-dicalciumphosphate and sodium pyrophosphate (1450 ppm F); 0.76% MFP and 0.33% NaF-silica (2500ppm F); non-fluoridated-silica (placebo) |
EFU were significantly higher with NaF dentifrices than MFP Ionic F dose-response was demonstrated pyrophosphate in the NaF dentifrices had no negative effects on F availability and did not interfere with the EFU |
|
Patil and Anegundi12 |
2014 |
Evaluate EFU with four different fluoride dentifrices |
60 extracted premolars |
Dentifrices: NaF, NaMFP, SnF2, AmF |
EFU in an increasing order was NaF < NaMFP < SnF2 < AmF EFU is higher at lower pH |
|
Cheng et al.25 |
2015 |
Evaluate the interaction of arginine and fluoride on the remineralization of artificial enamel carious lesions |
EFU determination (n=8 for each group) |
Dentifrices: 1400 ppm F; 1400 ppm F+8% arginine bicarbonate |
The ability of arginine to enhance fluoride absorption into demineralized lesions |
|
GlaxoSmithKline26 (company) |
2015 |
Evaluate enamel remineralization effect of experimental sodium fluoride-silica dentifrice formulations, with and without zinc |
53 participants completed the study |
Dentifrices: NaF (1426 ppm F), NaF (1150 ppm F), NaF (250 ppm F), NaF (1426 ppm F) + zinc base A, NaF (1426 ppm F) + zinc base B, Fluoride (0 ppm F) |
Dose-response was shown between many dentifrices EFU was slightly lower in dentifrices with zinc |
|
Creeth et al.15 |
2016 |
Determine the influence of toothbrushing duration and dentifrice quantity on fluoride efficacy |
52 participants completed the study |
Dentifrices- duration: 0.5 g of NaF (1150 ppm F)- 45 s 0.5 g of NaF (1150 ppm F)- 120 s 1.5 g of NaF (1150 ppm F)- 45 s 1.5 g of NaF (1150 ppm F)- 120 s 1.5 g of NaF (250 ppm F)- 120 s |
Increasing duration from 45 s to 120 s (1.5 g of 1150 ppm F dentifrice) increased FEU by 26.9%
Increasing the quantity from 0.5g to 1.5g (1150 ppm F dentifrice for 12s) increased EFU by 43%
Increasing F concentration from 250ppm to 1150ppm increased EFU by 114% |
|
Domenick Zero27 |
2018 |
Evaluate the F dose response of different dentifrices fluoride concentrations (0, 250, 500, 1100 ppm F) |
25 participants completed the study |
Dentifrices: 250 ppm NaF (dose-response control); 500 ppm NaF (dose-response control); 1100 ppm NaF (positive control) |
Higher EFU in relation with increased F concentration |
|
Parkinson et al.28 |
2018 |
Evaluate F mouth rinse used following fluoride or non-fluoride dentifrice |
52 participants completed the study |
Dentifrice: NaF (1150 ppm F) Mouth rinse: NaF (220 ppm F) |
The use of F dentifrice/F rinse increased the EFU significantly |
|
Parkinson et al.29 |
2018 |
Investigate the dose-response of phytate-containing 1150 ppm F dentifrice on model caries lesions and to determine the impact of zinc ions |
42 participants completed the study |
Dentifrices: 0.425% phytate/F; 0.85% phytate/F; 0.85% phytate/Zn/F; F-only; Zn/F and a 0% F placebo |
No difference in EFU between the F dentifrice with or without phytate
The presence of zinc does not impact fluoride efficacy |
|
Zero et al.30 |
2018 |
Investigate remineralization and F bioavailability in the enamel of dentifrice formulations with different F salts and combinations at 1400–1450 ppm F, different abrasive systems, and Carb |
Study 1 (N=57) Study 2 (N=63) Study 3 (N=82) |
Dentifrices: Study 1: NaF/Carb/silica, NaF/silica, NaF+MFP /chalk Study 2: NaF/Carb/silica, NaF+MFP/dical, AmF /silica Study 3: NaF/Carb/silica, NaF+SnF2/silica/ HMP. included Placebo (0 ppm F) and/or dose-response controls 675F-NaF±Carb |
Dose-response was shown between some dentifrices with a higher level of F (1400-1500) and medium level (675 ppm F) or no F NaF+SnF2/silica/ HMP performed significantly lower EFU than all active treatment NaF and AmF (as sole F source) dentifrices provides the greatest EFU The addition of Carb neither improved nor diminished EFU |
|
F Fluoride, NaF Sodium Fluoride, SnF2 Stannous Fluoride, NaMFP Sodium MonoFluoro Phosphate, AmF Amine Fluoride, CaCl2 Calcium Chloride, ppm parts per million, HMP Hexa Meta Phosphate, EFU Enamel Fluoride Uptake, s Seconds, g Grams, Zn Zinc, LBF Loosely Bound Fluoride, FBF Firmly Bound Fluoride, Carb Carbomer |
|||||
Table 1: Main findings of the included studies
Results
A total of 3572 study reports were identified from database searches. Only 34 articles were eligible for full-text retrieval. Of these, 22 articles were excluded as they failed to meet the inclusion criteria (Figure 1).
Fluoride formulations in dentifrices and EFU
Four research papers were published on multiple fluoride formulations. Patil & Anegundi (2014) compared the EFU in four different fluoride dentifrices with different F formulations in an in vitro analysis and pointed out that higher EFU was linked to samples treated with Amine F followed by those treated with SnF2, NaMFP and NaF.12 Inconsistent with the previous analysis, Arnold et al (2006) observed the higher EFU in AmF-treated samples followed by NaMFP and NaF respectively.14 Unlike two previous reports, Hattab (2013) considered EFU with NaF dentifrices substantially higher than MFP.24 While Zero et al (2018) reported that NaF and AmF in dentifrice were the sole F sources have a greater EFU than those of MFP or SnF2.30
The fluoride concentration of dentifrice (dose-response) and EFU
Four scientific articles analyzed the F concentration of dentifrice (dose-response) and fluoride enamel uptake. Creeth et al (2016) compared fluoride concentration of 250ppm and 1150ppm when brushing for 120s. The study finding indicated a 140% increase in EFU.15 Domenick Zero conducted a clinical trial (2018) and reported higher EFU with increased F concentration from 250ppm to 500ppm, and from 500ppm to 1100ppm.27 Moreover, results of a pooled analysis from three randomized trials established the dose-response and increased EFU between many dentifrices with a higher level of F (1400-1500 ppm) and medium level (675 ppm F) compared to the no Fluoride dentifrices. 30 Hattab (2013) evaluated EFU from eight dentifrices of various fluoride concentrations. A strong correlation was found between ionic F levels in dentifrices and their efficacy.24
Creeth et al (2016) also compared 45 seconds brushing duration to 120 seconds using 1.5 g of 1150 ppm F dentifrice; it was noted that EFU increased by 26.9% when brushing for 120 seconds. Furthermore, increasing the quantity from 0.5g to 1.5g of 1150 ppm F dentifrice increased EFU by 43%.15
Incorporation of phosphates to the fluoridated dentifrice and EFU
Three research papers were reviewed on phosphate incorporation. Zero et al (2018) used NaF+SnF2/silica/ HMP (which contains hexametaphosphate) dentifrice and found a significantly lower EFU than all active treatment.30 In contrast to HMP, the addition of pyrophosphate to NaF dentifrice showed no interference with EFU.24 Moreover, Parkinson, et al. (2018) reported no difference in EFU of the F dentifrice with or without phytate.29 Similarly, the presence of zinc in fluoridated dentifrices either did not interfere with fluoride efficacy or led to a slight decrease in the EFU.26, 28
The combined use of fluoridated mouth rinses with fluoridated dentifrices and EFU
Two publications analyzed the effect combined use of fluoridated mouth rinse and fluoridated dentifrice on EFU. It was observed that the EFU was significantly high when F rinse (220ppm) was used in conjugation with F dentifrice (1150ppm) compared to the use of dentifrice (1150ppm F) or F rinse (220ppm) alone.29 While in a study conducted by Úbeda et al (2005) pre-rinse with CaCl2 solution did not increase EFU from fluoridated dentifrices.22
pH variation and EFU
Two publications analyzed the effect of pH variability of the dentifrices and EFU. Patil and Anegundi (2014) observed that EFU was higher in samples treated with a lower pH (5.05, 5.34, 9.43, and 8.15, respectively).12 While Nobre-dos-Santos et al (2007) reported that the acidulated (pH 5.5) low-fluoride dentifrice (550ppm) had similar remineralization and firmly bound fluoride as neutral (pH 7) 1100ppm F dentifrice even after the concentration of F was low.23 On the contrary, Zero et al. (2018) found that the addition of Carbomer to the fluoridated dentifrice neither improved nor diminished EFU.28 However, the addition of arginine enhanced fluoride absorption into demineralized lesions.25
Discussion
Currently, manufacturers have renewed their interest in search of new fluoridated dentifrices to attain maximum effectiveness of fluoride ions to have an ideal cariostatic effect through uptake and diffusion of fluoride in demineralized enamel. It has been found that various factors related to the fluoridated dentifrice affect EFU and enamel remineralization. Hence this study reviewed the fluoride dentifrices and the factors affecting fluoride uptake by tooth enamel.
Most of the studies agreed that higher EFU is associated with the presence of Amine Fluoride, an organic fluoride within the dentifrice. This can be explained by the increased distribution of organic material in demineralized enamel. Amine Fluoride has a hydrophilic part that attaches to the tooth surface, and a hydrophobic part aligned toward the oral cavity; therefore, it prevents the saliva from washing it out rapidly. All other mentioned fluorides were inorganic compounds resulting in lower EFU.
EFU's dose-response influence was well known. By growing F concentration by around five times from 250ppm to 1150ppm, research published by Creeth et al (2016) noticed the EFU rise to 140% higher.15 Similar results were reported in the literature with different concentrations of F dentifrices.24, 27 Thus, higher concentrations of fluoride in dentifrices were proven to have a highly statistically significant effect in preventing dental caries.31 Generally, the use of 1000-1500ppm offers preventive benefits for caries; meanwhile, it is recommended to use 5000ppm of dentifrices in high-risk caries communities.
An increased brushing period enhances the potency of fluoride by improving F penetration into plaque and attaching to soft tissue thereby increasing the EFU and remineralization. However, most individuals fail to perform daily brushing over 120 seconds.32 Since brushing time and dentifrice quantity are related variables, 120 seconds of brushing with 1.5 g of dentifrice are recommended.15
Dentifrices generally have multiple functions other than caries prevention. One of these is to control extrinsic stains, which can be achieved by adding agents such as phosphates to inhibit the stain formation on dental enamel. Previous studies have confirmed that the addition of phosphates compounds, e.g., pyrophosphate and phytate, did not interfere with EFU dentifrice.24, 28 Meanwhile, the addition of hexametaphosphate was associated with lower EFU, which influence the remineralization ability of the dentifrice.30
Another function of dentifrices is to control malodor, which is achieved by adding zinc ions as they have an antimicrobial effect and ability to bind to the volatile sulfur compounds produced by anaerobic bacteria in the oral cavity.33 Studies have reported slight or no effect zinc ions on EFU.27, 28 Hence further investigations are required in this area.
EFU after brushing with F dentifrices is known to depend on the CaCl2 compound as it serves as a reservoir of F release as pH decreases.22 It is desirable to use F mouth rinse in combination with F dentifrice to achieve additive caries preventive benefits to provide a 23% higher caries reduction.17, 29
Despite a lack of information regarding the mechanism by which decreasing the pH enhances the EFU and, therefore, the anticaries effect of dentifrices, it has been proven that acidulated dentifrices are more effective than neutral ones. It can have a significant role in decreasing the risk of fluorosis by reducing the concentration of F in children's dentifrices concurrently, obtaining the anticaries effect by lowering the pH. 23
The addition of Carbomer and arginine to dentifrices was tested with regards to EFU and remineralization. Arginine is one of the components of human saliva that oral bacteria catabolize to ammonia, leading to increased pH and equilibrium of the oral microbial environment. Furthermore, it has been suggested that the addition of arginine to dentifrices reduces the hypersensitivity by facilitating dentinal tubule occluding. Besides, Cheng et al. (2015) showed that it could increase EFU from dentifrices.25 In a similar study, incorporation of Carbomer to the dentifrices did not demonstrate any positive or negative effect on EFU and remineralization.30
The limitation of this review was that it included heterogeneous studies, the inclusion of only English literature, and the inclusion of studies published between 2005 to 2020. Due to a lack of confirmative data, more studies investigating CaCl2 mouth rinse, the effect of adding Carbomer and zinc on EFU would be interesting to consider for future research.
Conclusion
Within the limitations, this review highlights that the EFU from fluoridated dentifrices depends on several factors, including the range of F compounds, F concentration, pH of dentifrice, usage of mouth rinse, length of brushing, dentifrice quantity, and other added ingredients of the dentifrices. However, further studies are required to assess the effects of some other active agents of the dentifrices on the EFU.
References
Corresponding Author
Mohammad Abdul Baseer
Department of Preventive Dental Sciences,
College of Dentistry, Riyadh Elm University
Riyadh, Saudi Arabia
Email: basheer.dr @ gmail.com







