THE RELATIONSHIP BETWEEN CERVICAL SPINE ABNORMALITIES AND TEMPOROMANDIBULAR JOINT INTERNAL DISORDERS: A SYSTEMATIC REVIEW OF LITERATURE
Zygimantas Petronis1*, Ieva Pliatkute1, Audra Janovskiene1, Marijus Leketas1
1Department of Maxillofacial Surgery, Lithuanian University of Health Sciences, Kaunas Lithuania. [email protected]
https://doi.org/10.51847/sGUN5P9OQA
ABSTRACT
Changes in head and neck posture may affect the function of the jaw and masticatory muscles, as well as the range of motion of the neck and the activity of the cervical muscles in temporomandibular disorder (TMD) patients. This systematic review was performed according to Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was carried out using the advanced features of PubMed, ResearchGate, Cochrane Library, Scopus, and Google Scholar databases. “Cervical spine”, “temporomandibular joint”, and “pain” are the keywords that were used in the search strategy.
A total of 273 articles were included in the title and abstract screening. After the eligibility process, 52 records were obtained, and the full texts of the related studies were read. Finally, a total of 6 articles fulfilled all necessary inclusion criteria in this systematic review. A total of 417 patients were potential participants in TMD-related clinical trials, of which 302 patients were included in intervention groups. Decreased side flexion, increased TMD-related pain intensity, a higher number of active trigger points in masticatory and cervical muscles, and reduced C0-C1 distance were found to significantly impact TMJ-related cervical abnormalities.
Key words: Cervical spine abnormalities, Temporomandibular joint, Internal disorders, Relationship, Craniocervical mandibular system.
Introduction
Temporomandibular disorders (TMDs) are a group of diseases that affect the masticatory muscles, the temporomandibular joints (TMJs), and the structures around them [1]. The "craniocervical-mandibular system," which consists of the temporomandibular joint, the masticatory muscles, and ligaments connecting the temporomandibular joint and the cervical region, is a functional unit that has yet to be fully understood [2]. However, this biomechanical interaction may play a role in the functional reliance between the cervical and masticatory systems [3]. Studies have covered the tight connection between TMD and cervical diseases many times [4, 5]. Changes in head and neck posture may affect the function of the jaw and masticatory muscles, as well as the range of motion of the neck and the activity of the cervical muscles in TMD patients [4]. TMD symptoms can co-occur with other conditions such as neck and shoulder pain and related headaches [5].
One of today's most prevalent medical problems is back pain. Back pain symptoms may manifest due to several pathologies and reasons [6]. According to the literature, 43% of women and 30% of men have had neck pain at some point in their lives, and the pain intensity becomes worse as people get older [7]. Speaking about TMD, the risk is more than twice as high for women than for men. However, additional equally crucial factors that have been recently described in the literature must also be taken into consideration. These include self-rated general health conditions, general chronic pain disorders, age, study site, ethnicity, psychosocial factors, and genetic factors [8]. Other sources state that the prevalence of chronic TMD is 1.6% (men 1.3%, women 1.8%), and chronic TMD persists to negatively impact the quality of life [9].
To assess the functional and dysfunctional components of the craniocervical mandibular system, anatomical links among the studied structures are examined because it is impossible to capture functions in real-time as they are performed [10]. Numerous investigations have established a connection between the cranial area, the temporomandibular joint, the cervical spine, and the hyoid bone in terms of both morphological and functional relationships [11, 12]. Neck pain and headaches are frequently accompanied by temporomandibular problems [5]. The link between TMD and alterations in head and neck posture is still debatable and uncertain, which is why it has been decided to check on the relationship between cervical spine abnormalities and TMJ dysfunctions [13].
Materials and Methods
This systematic review was performed according to Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines [14]. The authors registered the protocol in the International Prospective Register of Systematic Reviews under the number CRD42022330126. The following PICO strategy was established:
The PICO question leading the review was: “Are there any relations between cervical spine abnormalities and TMJ dysfunctions?”
Search strategy
A comprehensive literature search was carried out using the advanced features of PubMed, ResearchGate, Cochrane Library, Scopus, and Google Scholar databases. “Cervical spine”, “temporomandibular joint”, and “pain” are the keywords that were used in the search strategy. The literature search was restricted to articles written in English language and published within the past 5 years, from July 2017 to 2022. No search limitations concerning publication country or status were applied.
Selection criteria
The inclusion criteria included randomized controlled trials, as well as comparative, observational, retrospective studies, single-blinded, split-mouth randomized studies, and controlled clinical trials, in adult patients that compared the relationship of cervical spine abnormalities and TMJ disorders. The patients were older than 18 years old, complained of chronic orofacial pain, and were diagnosed with TMDs.
Exclusion criteria
Quality assessment
The Cochrane Collaboration tool for assessing the risk of bias was used to evaluate the quality of the selected studies. A total of seven domains were analyzed: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other potential threats to validity. Each component was classified as low-risk, unclear-risk, or high-risk.
Results and Discussion
Study selection
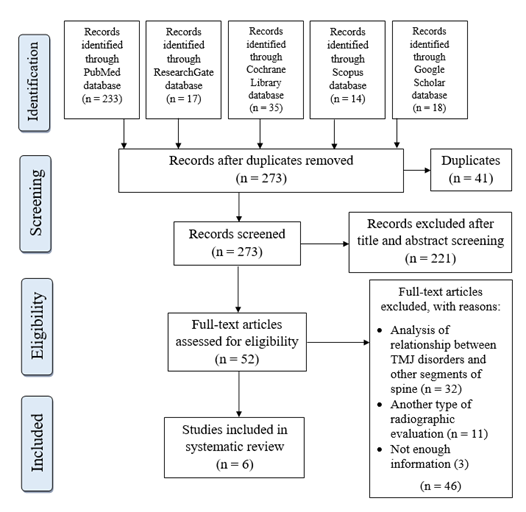
The electronic and manual search of the literature yielded 317 articles, of which 41 were duplicates and were excluded. A total of 273 articles were included in the title and abstract screening. After the eligibility process, 52 records were obtained and the full texts of the related studies were read. Finally, a total of 6 articles fulfilled all necessary inclusion criteria in this systematic review (Figure 1). The included studies were quantitatively and qualitatively analyzed. The main characteristics of included studies are summarized in Table 1.
|
|
|
Figure 1. PRISMA flow chart. |
Table 1. Characteristics of included studies.
|
Article |
Groups |
Diagnostic method |
Outcomes |
Intervention |
Treatment outcomes |
Study groups |
|||||||||
|
Control |
Study |
P value |
|||||||||||||
|
Kim et al. (2019) [15] |
Patients with fusion, posterior arch defect, and the presence of both abnormalities |
RDC/TMD |
Pain intensity, CMO, MMO, MOL, pain on opening, pain on capsule palpation, pain on masticatory muscle palpation |
Counseling, stress management, control of contributing factors, physical therapy (moist hot pack application, ultrasound, electric stimulation, occlusal splints, non-steroidal anti-inflammatory drugs) for 1 year |
|
Fusion abnormalities (with (n=10) / without (n=33)) |
Posterior arch deficiency (with (n=8) / without (n=35)) |
Presence of any abnormalities in TMJ (with (n=15) / without (n=28)) |
|||||||
|
Before treatment |
After treatment |
Before treatment |
After treatment |
Before treatment |
After treatment |
||||||||||
|
Pain intensity 1 |
3.7 (SD 2.9) / 4.0 (SD 2.7) |
0.3 (SD 0.7) / 0.9 (SD 1.6) |
4.1 (SD 3.6) / 3.9 (SD 2.5) |
1.0 (SD 1.7) / 0.7 (SD 1.4) |
4.3 (SD 3.2) / 3.9 (SD 2.5) |
0.7 (SD 1.4) / 0.8 (SD 1.5) |
|||||||||
|
P=0.781 |
P=0.096 |
P=0.856 |
P=0.645 |
P=0.671 |
P=0.806 |
||||||||||
|
The CMO ranges (mm) 1 |
35.8 (SD 9.2) / 40.2 (SD 9.4) |
44.9 (SD 10.7) / 45.6 (SD 7.3) |
33.3 (SD 9.1) / 40.7 (SD 9.0) |
39.5 (SD 9.4) / 46.7 (SD 7.2) |
35.4 (SD 9.3) / 41.2 (SD 9.0) |
43.0 (SD 10.1) / 46.7 (SD 6.6) |
|||||||||
|
P=0.217 |
P=0.828 |
P=0.044* |
P=0.020* |
P=0.057 |
P=0.216 |
||||||||||
|
The MMO ranges (mm) 1 |
42.9 (SD 9.9) / 44.9 (SD 7.8) |
45.5 (SD 9.7) / 46.7 (SD 7.0) |
39.8 (SD 6.9) / 45.5 (SD 8.2) |
40.9 (SD 7.9) / 47.7 (SD 7.1) |
42.2 (SD 9.3) / 45.6 (SD 7.6) |
43.8 (SD 9.0) / 47.8 (SD 6.5) |
|||||||||
|
P=0.513 |
P=0.676 |
P=0.075* |
P=0.021* |
P=0.200 |
P=0.144 |
||||||||||
|
The MOL ranges 2 |
3/10 (30.0%) / 8/33 (24.2%) |
3/10 (30.0%) / 5/33 (15.2%) |
3/8 (37.5%) / 8/35 (22.9%) |
4/8 (50%) / 4/35 (11.4%) |
5/15 (33.3%) / 6/28 (21.4%) |
6/15 (40.0%) / 2/28 (7.1%) |
|||||||||
|
P=0.698 |
P=0.362 |
P=0.401 |
P=0.028* |
P=0.473 |
P=0.014* |
||||||||||
|
Masticatory muscle palpation 2 |
8/10 (80.0%) / 21/33 (63.6%) |
3/10 (30.0%) / 12/33 (36.4%) |
6/8 (75.0%) / 23/35 (65.7%) |
6/8 (75.0%) / 9/35 (25.7%) |
12/15 (80.0%) / 17/28 (60.7%) |
7/15 (46.7%) / 8/28 (28.6%) |
|||||||||
|
P=0.456 |
P=0.711 |
P=0.613 |
P=0.014* |
P=0.308 |
P=0.235 |
||||||||||
|
Pain on opening 2 |
7/10 (70.0%) / 18/33 (54.5%) |
2/10 (20.0%) / 5/33 (15.2%) |
5/8 (62.5%) / 20/35 (57.1%) |
2/8 (25.0%) / 5/35 (14.3%) |
10/15 (66.7%) / 15/28 (53.6%) |
3/15 (20.0%) / 4/28 (14.3%) |
|||||||||
|
P=0.480 |
P=0.656 |
P=0.782 |
P=0.597 |
P=0.407 |
P=0.680 |
||||||||||
|
Pain on capsule palpation 2 |
5/10 (50.0%) / 13/33 0(39.4%) |
1/10 (10.0%) / 5/32 (15.6%) |
3/8 (37.5%) / 15/35 (42.9%) |
1/7 (14.3%) / 5/35 (14.3%) |
7/15 (46.7%) / 11/28 (39.3%) |
1/14 (7.1%) / 5/28 (17.9%) |
|||||||||
|
P=0.717 |
P=0.657 |
P=0.782 |
P=1.000 |
P=0.640 |
P=0.645 |
||||||||||
|
Calixtre et al. (2018) [16] |
61 women with TMD were randomized into an IG and a CG. |
RCD/TMD |
Primary: orofacial pain intensity, current, maximum, minimum pain. Secondary: pain sensitivity, functionality, headache impact. |
IG received upper cervical mobilizations and neck motor control and stabilization exercises for 5 weeks. |
|
Baseline |
Follow-up |
||||||||
|
CG |
SG |
CG |
SG |
||||||||||||
|
Curr. Pain |
3.1 (SD 2.7) |
4.0 (SD 2.6)* |
3.1 (SD 2.3) |
2.1 (SD 2.2)* |
|||||||||||
|
Max. pain |
6.2 (SD 1.7) |
6.1 (SD 2.1)* |
5.8 (SD 2.2) |
4.0 (SD 2.4)* |
|||||||||||
|
Min. pain |
1.5 (SD 1.5) |
1.9 (SD 1.7)* |
1.6 (SD 1.6) |
1.1 (SD 1.4)* |
|||||||||||
|
PPT temp. |
1.2 (SD 0.4) |
1.3 (SD 0.7) |
1.3 (SD 0.5) |
1.4 (SD 0.5) |
|||||||||||
|
PPT mass |
1.1 (SD 0.4) |
1.1 (SD 0.6) |
1.1 (SD 0.5) |
1.2 (SD 0.5) |
|||||||||||
|
HIT-6 |
62.5 (SD 6.1) |
61.4 (SD 6.0)* |
60.0 (SD 6.6) |
52.1 (SD 8.5)* |
|||||||||||
|
Wiest et al. (2019) [17] |
Group without TMD (n=37), group with low TMD (n=19), and group with moderate TMD (n=15). |
RDC/TMD |
Head position angle, cervical lordosis angle, dorsal kyphosis angle, lumbar lordosis angle |
NM |
Postural variable |
Group without TMD |
Group with TMD I – Low |
Group with TMD II – Moderate |
P value |
||||||
|
Head position angle (°) |
53.2±5.3 |
53.5±5.5 |
53.4±4.1 |
0.986 |
|||||||||||
|
Cervical lordosis angle (°) |
41.7±11.1+ |
43.6±6.7 |
49.5±7.8+ |
0.034 * |
|||||||||||
|
Dorsal kyphosis angle (°) |
44.1±9.3 |
43.1±5.8 |
49.1±6.5 |
0.070 * |
|||||||||||
|
Lumbar lordosis angle (°) |
46.5±5.2 |
45.1±4.9 |
45.9±6.6 |
0.659 |
|||||||||||
|
Benlidayi et al. (2018) [18] |
No control group |
60 patients with TMD |
RDC/TMD |
Neck pain, TMD-related variables (masticatory efficiency, functional limitation, pain score, depression score, disability points), cervical spinal variables (C2-C7 angle, flexion, extension, rotation right/left, side flexion right/left), NPDS |
NM |
|
Neck pain (-) (n=32) |
Neck pain (+) (n=28) |
Total (n=60) |
||||||
|
Masticatory efficiency (0-4) a |
2 (0–3) |
3 (0–4) ** |
2 (0–4) |
||||||||||||
|
Functional limitation (0-4) a |
2 (0-4) |
3 (0-4) |
2 (0-4) |
||||||||||||
|
Pain score (0-100) b |
50.1 ± 21.8 |
63.7 ± 18.6* |
56.4 ± 2.1 |
||||||||||||
|
Depression score (0-4) b |
0.9 ± 0.7 |
1.4 ± 0.7** |
1.2 ± 0.7 |
||||||||||||
|
Disability points (0-4) a |
0 (0-3) |
1 (0-4) |
0 (0-4) |
||||||||||||
|
C2-C7 angle (°) b |
9.8 ± 12.7 |
12.2 ± 12.8 |
10.9 ± 12.7 |
||||||||||||
|
Flexion (°) b |
60 (40-60) |
50 (35-70) |
55 (35-70) |
||||||||||||
|
Extension (°) b |
45 (30–60) |
40 (30–60) |
45 (30–60) |
||||||||||||
|
Rotation right (°) b |
60 (35–80) |
50 (30–80) |
60 (30–80) |
||||||||||||
|
Rotation left (°) b |
60 (40–80) |
55 (40–80) |
60 (40–80) |
||||||||||||
|
Side flexion right (°) b |
45 (35–60) |
40 (30–50) ** |
45 (30–60) |
||||||||||||
|
Side flexion left (°) b |
45 (30–60) |
40 (30–50) ** |
45 (30–60) |
||||||||||||
|
Giacomo et al. (2018) [19] |
Group B – 33 patients without dysfunctions |
Group A – 26 patients with dysfunctions |
DC/TMD |
C0-C1 and C1-C2 distance values, hyoid bone position, craniocervical angle value |
NM |
|
TMD |
ANB value |
Abnormally low (<4.5mm) |
Normal |
Abnormally high (>4.5mm) |
||||
|
C0-C1 distance value |
Absent (n=33) |
5 to 9 |
3 (9%) |
23 (70%) |
7 (21%) |
||||||||||
|
Present (n=26) |
9 (35%) |
15 (58%) |
2 (8%) |
||||||||||||
|
C1-C2 distance value) |
Absent (n=33) |
5 to 9 |
4 (12%) |
24 (73%) |
5 (15%) |
||||||||||
|
Present (n=26) |
6 (23%) |
19 (73%) |
1 (4%) |
||||||||||||
|
Hyoid bone position |
Absent (n=33) |
5 to 9 |
15 (45%) |
18 (55%) |
- |
||||||||||
|
Present (n=26) |
14 (54%) |
12 (46%) |
- |
||||||||||||
|
Craniocervical angle value |
Absent (n=33) |
5 to 9 |
18 (55%) |
13 (39%) |
2 (6%) |
||||||||||
|
Present (n=26) |
12 (46%) |
13 (50%) |
1 (4%) |
||||||||||||
|
Hong et al. (2019) [20] |
45 patients, who showed no signs of myofascial TMD or cervical pain |
26 patients with myofascial TMD (mTMD); 49 patients with both myofascial TMD and cervical pain (cerTMD) |
RDC/TMD |
CMO, MMO, VAS from TMD, number of active/latent trigger points in masticatory/cervical muscles |
NM |
|
CG (n=45) |
mTMD (n=26) |
cerTMD (n=49) |
P value |
|||||
|
CMO (mm) |
45.0 ± 5.9 |
44.2 ± 7.2 |
41.0 ± 7.4 |
0.016 * |
|||||||||||
|
MMO (mm) |
45.3 ± 5.1 |
45.7 ± 6.6 |
42.8 ± 6.8 |
0.021 * |
|||||||||||
|
VAS from TMD |
0 |
5.12 ± 2.47 |
6.78 ± 2.75 |
< 0.001 *** |
|||||||||||
|
Number of active trigger points in masticatory muscles |
0 |
1.65 ± 1.32 |
2.47 ± 1.60 |
< 0.001 *** |
|||||||||||
|
Number of active trigger points in cervical muscles |
0 |
1.15 ± 1.76 |
5.10 ± 3.18 |
< 0.001 *** |
|||||||||||
|
Number of latent trigger points in masticatory muscles |
0 |
0.62 ± 0.85 |
0.71 ± 1.15 |
0.096 |
|||||||||||
|
Number of latent trigger points in cervical muscles |
0 |
0.04 ± 0.30 |
1.04 ± 1.93 |
< 0.001 *** |
|||||||||||
|
C0-C1 distance |
26.3 ± 8.3 |
25.8 ± 8.4 |
22.3 ± 6.6 |
0.019 * |
|||||||||||
|
C1-C2 distance |
39.6 ± 8.9 |
32.9 ± 8.1 |
31.3 ± 9.9 |
< 0.001 *** |
|||||||||||
RDC/TMD: Research Diagnostic Criteria for Temporomandibular Disorders; MMO: maximum mouth opening; CMO: comfortable mouth opening; MOL: mouth opening limitation; VAS: visual analog scale; NM: not mentioned; PPT: pressure pain threshold; temp: temporalis; mass: masseters.
*Significant difference (P<0.05)
** P<0.01)
*** P<0.001
1 – Differences between groups were tested with a t-test.
2 – Differences between groups were tested with a chi-square test.
a – values represented median (minimum-maximum)
b – values represented mean ± standard deviation
Characteristics of included studies
This systematic review included observation [17] and cross-sectional [20] studies, a single-blind randomized controlled trial [16], a research article [19], and two studies [15, 18] that did not specify their type of study.
Risk of bias within the studies
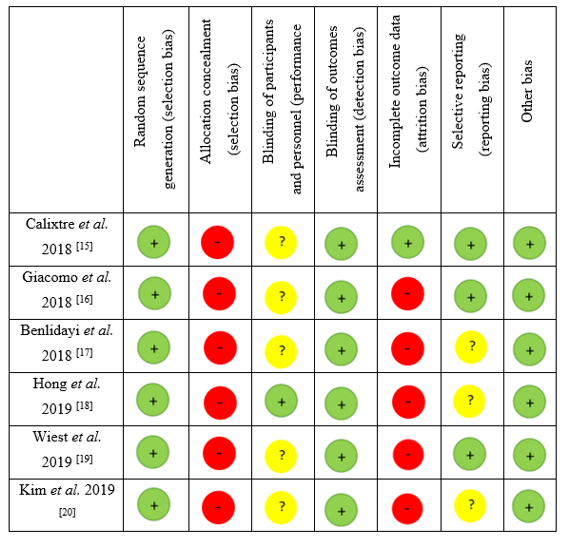
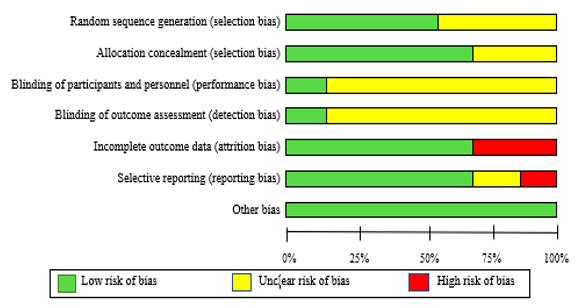
All 6 included studies were evaluated qualitatively by the tools of Cochrane Collaboration for the risk of bias (Figure 2). The assessment of the risk of bias was carried out independently by two reviewers. Two studies [17, 19] had a high risk of bias in incomplete outcome data. A high risk of bias in selective reporting was observed only in a study by Wiest et al. [17]. The highest proportion of low risk of bias included other biases, allocation concealment, incomplete outcome data, and selective reporting. Meanwhile, blinding of participants and personnel, and blinding of outcome assessment were noted as the highest proportion of unclear risk bias.
|
|
|
a) |
|
|
|
b) |
|
Figure 2. Risk of bias assessment of included studies in the review. a) Risk of bias summary; b) Risk of bias graph. Symbols. (+): low risk of bias; (?): unclear risk of bias; (-): high risk of bias |
Clinical characteristics of TMD patients
A total of 417 patients were potential participants in TMD-related clinical trials, of which 302 patients were included in intervention groups. TMJ dysfunctions were diagnosed according to the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) method. RDC/TMD is a widely used diagnostic method for TMD assessment and it is conducted of two components: Axis I, which is used for a clinical and radiographic evaluation of myofascial pain, disc displacement, arthralgia, arthritis, arthrosis, and Axis II, for psychologic status and pain-related disability [21, 22]. Disorders, such as orofacial myalgia or myofascial pain, disc displacement with reduction, decreased jaw movement amplitudes and side flexions to both sides, the presence of cracking or crackling of the movement, arthralgia, osteoarthrosis, were considered as TMJ-related disorders [15-20].
Clinical assessment between TMD and cervical spine abnormalities
A study by Calixtre et al. [16] observed 61 women patients who were randomly selected for interventional (IG) and control groups (CG). The IG received 10 sessions of physiotherapy over 5 weeks, twice a week within at least 48 hours apart. The following outcomes were divided into primary and secondary (pain sensitivity and functionality) outcomes. Orofacial pain intensity has significantly decreased (P<0.05) only in the IG after 5 weeks of treatment aimed at the upper cervical spine compared with the CG. A significant interplay (P<0.05) in headache impact according to HIT-6 was observed in the IG group in both time frames. No statistically significant effect was obtained for PPT of the masticatory and temporal muscles after the treatment.
Giacomo et al. [19] used the integrated DC/TMD according to the presence or not of dysfunctions of TMJ to divide patients into two subgroups. A study group consisted of patients with the following disorders, disc displacement with reduction, myalgia, and myofascial pain, subluxation, headache associated with TMD, arthralgia, and osteoarthrosis. To evaluate the relationship between TMD and cervical spine abnormalities, cephalometric assessment of C0-C1 and C1-C2 distance value, hyoid bone position, and craniocervical angle value was used. No statistically significant difference between the decrease or increase of ANB value in both groups was found.
In a study by Benlidayi et al. [18] 60 patients with TMD and with the presence or not of neck pain were evaluated according to the RDC/TMD. A significant difference between the results was found only among patients with neck pain. TMD-related masticatory efficiency (P<0.01), pain score (P<0.05), and depression score (P<0.01) were significantly higher in patients with neck pain compared to patients without neck pain. Additionally, side flexion to both sides was significantly lower (P<0.01) in patients with neck pain compared to patients without neck pain. However, functional limitation, disability points, C2-C7 angle, flexion, extension, and rotation to both sides showed no statistically significant difference between patients with or without neck pain, thus TMJ dysfunctions were not correlated with cervical abnormalities.
Hong et al. [20] classified patients into three groups: patients with no signs of TMD (control group), patients with myofascial TMD (mTMD), and patients with both myofascial TMD and cervical pain (cerTMD). The comfortable and maximum mouth opening was significantly decreased in the cerTMD group compared to the control and mTMD groups (P<0.05). TMD-related pain intensity and the number of active trigger points in masticatory and cervical muscles were considerably higher in the cerTMD group compared to the control and mTMD groups (P<0.001). The distance of the cranium-atlas (C0-C1) and atlas-axis (C1-C2) were measured to assess the head and neck posture [23]. A significant decrease in the distance of C0-C1 and C1-C2 was observed in both mTMD and cerTMD groups (P<0.05 and P<0.001 respectively), but the lowest distance was found in the cerTMD group. The reduction of the C0-C1 distance indicates posterior rotation of the cranium.
A study by Wiest et al. [17] divided 71 patients into three groups: without TMD, with low TMD, and with moderate TMD. The previously mentioned group had a significantly higher cervical lordosis and dorsal kyphosis angle (P<0.05) compared to the group without TMD and the group with low TMD. It was presented as a weak and significant correlation with the severity of TMD. No statistically significant difference between head position angle and lumbar lordosis angle was observed in cervical spine abnormalities and TMD.
In a study by Kim et al. [15] a total of 43 patients clinically diagnosed with TMD obtained a conservative treatment for more than one year. The presence of fusion abnormalities, posterior arch deficiency (PAD), or the presence of both abnormalities was considered as upper cervical spine abnormalities. An increased comfort and maximum range of mouth opening after treatment was found in all three groups, however, a significantly improved result was observed in the PAD group (P<0.05). The mouth opening limitation ranges have significantly enlarged after the treatment in the PAD and the presence of any abnormalities of TMJ groups (P<0.05). The decrease in pain on masticatory muscle palpation after the treatment in the two groups did not show a significant difference, however, a positive response was observed in the PAD group after the treatment (P=0.014). No statistically significant correlation was found in pain intensity, pain on opening, or capsule palpation between groups after the treatment.
Statistical analysis
Firstly, a systematic review and meta-analysis (qualitative and quantitative analysis) were planned. No quantitative analysis (meta-analysis) could be performed due to the high heterogeneity of the data. As a result, the systematic review only conducted a descriptive analysis of the retrieved information, without a quantitative assessment, to identify and analyze relevant data for statistical significance. Statistical data was expressed using the mean and standard deviation (M ± SD).
The goal of this systematic review was to assess the relationship between cervical spine abnormalities and TMJ dysfunctions, and to examine the functional and dysfunctional components of the craniocervical mandibular system. 8 articles were selected for this review according to predefined eligibility criteria. Due to the high methodological heterogeneity between the studies, the meta-analysis was not performed. However, the qualitative analysis revealed that decreased side flexion [18], TMD-related pain intensity, the higher number of active trigger points in masticatory and cervical muscles, reduction of C0-C1 distance [20], higher cervical lordosis and dorsal kyphosis angle [17] can significantly impact TMD related cervical abnormalities, as well as a 1-year conservative treatment can significantly reduce the TMD related symptoms [15].
Walczynska-Dragon et al. [24] study, along with clinical follow-up, indicates a high frequency of TMD coexisting with cervical spine pain. The key finding from the described study is the significant improvement in range of motion (ROM) in the cervical spine and the elimination of cervical spine pain experienced by subjects in the experimental group. Based on these study results, it becomes evident that interdisciplinary cooperation among orthopedists, laryngologists, neurologists, and dentists is necessary and essential.
The presented study did not evaluate cervical spine abnormalities and TMJ dysfunctions in relation to bruxism. However, according to Piekartz, H.v., et al. [25], their study revealed that female subjects with bruxism have more features of myofascial TMD according to the DC/TMD consortium criteria. However, it is important to note that their study did not make direct observations regarding the relationship between bruxism and TMD. Nonetheless, the research findings demonstrated that bruxism and the severity of TMD are independent predictors for pain and cervical disability, as assessed by the Neck Disability Index (NDI) score. Interestingly, the study also found that physical measurements showed a strong relationship with pain variables, but not with variables related to ROM. These findings hold significance for clinical practice, suggesting that clinicians may encounter painful cervical clinical tests in individuals with bruxism, which may not be directly attributed to problems in the craniocervical region due to a lack of cervical impairments.
However, in our study, the treatment effects were not directly observed. It is important to note that Calixtre LB et al. [26], research has provided valuable insights. According to their findings, compared to the baseline, a significant improvement in myofascial pain and mouth opening was observed following manual therapy treatment in cases with myogenous-TMD. The short-term analysis of existing data suggests that manual therapy is an effective treatment option for TMD. Specifically, mobilization and manipulation of the upper cervical spine were found to be preferable approaches. However, it is important to acknowledge that there is limited high-quality evidence available to determine the optimal procedure or combination of manual therapy approaches and treatment duration for TMD conditions. A similar statement is made by Alan C. Lam et al. [27], who state that the current understanding of TMD lacks a standardized treatment approach, leading clinicians to employ a multimodal care strategy encompassing education, exercise, and manual therapy. In this regard, clinicians often view the cervical spine as a potential source of TMJ symptoms. Previous systematic reviews, including those conducted by Alan C. Lam et al. [27], have investigated the efficacy of various cervical manual therapy techniques for TMJ dysfunction, such as myofascial release targeting the masticatory and cervical muscles, mobilization/manipulation of the cervical and thoracic spine, and combined interventions. Furthermore, TMJ dysfunction has been associated with poor quality of sleep and exposure to stressful life events, particularly when muscular pain is involved. Clinical heterogeneity among trials may arise from factors such as psychological overlay, chronic stress, pain duration, and patient-specific beliefs and expectations regarding care. This heterogeneity may have a greater impact on subjective outcomes, which could explain the variability observed in subjective pain ratings and pressure pain thresholds (PPTs) of the masseter and temporalis muscles compared to measurements of maximal mouth opening. Nevertheless, despite small effect sizes and substantial heterogeneity, meaningful effects can still be derived from specific interventions.
Conclusion
This systematic review aimed to investigate the relationship between cervical spine abnormalities and temporomandibular joint (TMJ) dysfunctions. Decreased side flexion, increased TMD-related pain intensity, a higher number of active trigger points in masticatory and cervical muscles, and reduced C0-C1 distance were found to significantly impact TMJ-related cervical abnormalities. Additionally, conservative treatment over one year showed significant improvement in TMJ symptoms. These findings highlight the complex interplay between the cervical spine and TMJ and emphasize the need for interdisciplinary collaboration in managing patients with TMD and cervical spine pain. Further research is warranted to explore the influence of bruxism on TMD and cervical dysfunction.
Acknowledgments: We would like to acknowledge the help of Lithuanian University of Health Sciences.
Conflict of interest: None
Financial support: None
Ethics statement: This study fulfils the ethical requirements of Lithuanian University of Health Sciences.