
SALIVARY COPPER AND ZINC LEVELS IN DENTAL CARIES: AN EXVIVO STUDY
Nireeksha1*, Mithra N Hegde2, Suchetha Kumari N3, Shilpa Shetty4
1 Lecturer, Department of Conservative Dentistry and Endodontics, A.B. Shetty Memorial Institute of Dental Sciences, Nitte University, (Deemed to be), Deralakatte Mangalore, 575018.
2 Vice-principal, Head of the Department, Department of Conservative Dentistry and Endodontics, A.B.Shetty Memorial Institute of Dental Sciences, Nitte University, (Deemed to be), Deralakatte Mangalore, 575018.
3 Professor, Department of biochemistry, Principal scientific officer, Central research laboratory, K.S.hegde medical academy, Nitte University (Deemed to be), Deralakatte, Magalore, 575018.
4 Research assistant, Central Research Laboratory, K.S.hegde medical academy, Nitte University (Deemed to be), Deralakatte, Magalore, 575018.
|
|
Introduction
Among oral diseases, dental caries is the most common chronic disease of humankind 1. The salivary fluid is an important physiologic fluid and it is considered as a diagnostic agent 2. The composition of saliva is vastly studied as it provides valuable insight into the biochemical and physiological processes of various diseases 3, 4. Various components of saliva are studied in relationship with dental caries. The practice of dentistry is associated with one of the high levels of occupational stress 5. Dental Implants is important dentistry in recent years 6. The ease of collection quantification helps us easily identify various elements that yield a strong association between their presence, absence, and occurrence of particular pathology or diseases 7. Saliva due to its extensive association with all the tissues in the oral cavity seems as potent indicators for various elements. Thus any types of changes in salivary levels of these measurable elements can be considered a potential indicates and biomarker for occurrence/progression disease condition 8, 9.
Trace elements are present in minute quantities in saliva. They play a major role in various metabolic processes>25% of enzymes need these metal ions/trace elements for their activation 10. Various authors mentioned that microelements/trace elements in saliva are directly related to caries occurrence along with other factors 11, 12. Non-stimulated saliva shows osmolarity equivalent to half of the plasma osmolarity also there is an equilibrium between the component that is present in saliva and on the tooth surface 13. The most important trace element that has a role to play in the pathogenesis of dental caries are Ca, Na, Zn, Mg, Fl 14.
Salivary zinc levels show variation significantly in the presence or absence of a pathological process. Zinc plays a major role in the activation of various enzymes. Also, the outer layer of the tooth is affected by zinc approximately up to 200-900 ppm than the inner layer. It is always shown to enhance remineralization of enamel 15. Zinc plays a major role in bacterial adhesion, growth, and bacterial activity inhibition. In biofilm models, zinc competes with calcium for binding sites therefore also has been shown that the zinc concentration pre and post-eruption increases this suggests zinc incorporation occurs 16. The incorporated zinc, part by part is released under the acidic condition from the tooth surface through carboxylate protonation and sources of phosphate groups in bacteria.17
Copper is an essential trace element for different metabolic processes and enzyme activities 18. Copper has been shown to have cariostatic action in rat models, which is mainly due to oxidizing key thiol groups of enzymes crucial for bacterial metabolism, thereby it prevents plaque formation and degradation of acids on exposure to sugar 19, 20. It was also shown in the studies that the topical application of copper form copper phosphate layer that is acid insoluble 20.
This study aims to evaluate the salivary zinc and copper levels in association with dental caries.
Material and Methods:
After obtaining the ethical clearance the salivary samples were collected from 60 individuals who were eligible based on the inclusion criteria. The individuals included in the study were under the age group of 18 to 40 years, free from systemic and local illness that affects the salivary flow. Individuals with a systemic illness like diabetes, Rheumatoid arthritis, undergoing radiotherapy individuals with chronic generalized gingivitis and periodontitis, under Long-term medication for illness and individuals under a restricted diet were excluded from the study. Further oral examination was done based on which individuals were classified as caries-free and caries active individuals.
Oral examination: Mouth mirror and the straight probe was used to perform a clinical evaluation, patients seated on the dental chair. Dental caries evaluation: “D” in the DMFT index determines the no. of a decayed tooth. The patient was seated in the dental chair, under the ideal illumination mouth mirror and the straight probe was used to evaluate caries and recorded in the WHO oral survey2013 format. Any probe, catch or caries involving to any extent was coded as “D”
Individuals were further divided into caries active and caries-free group based on the no.of decayed tooth present. Individuals with caries; caries active group (D=more than 4) and absence of caries; caries-free group(D=0).
Biochemical analysis: Unstimulated saliva samples were collected by Navazesh Protocol. Subjects were asked to abstain from smoking brushing of teeth, use of mouthwash, eat/drink for 2 hours before the sample collection. The sample was collected between 10.00 am – 11.00 am.
During the sample, collection subjects were seated in a normal chair instead of the dental chair to maintain a stress-free environment. Once saliva is pooled on the floor of the mouth 5 ml was collected in a Tarson’s saliva collection tube. Five milliliters of saliva was collected from the patient, centrifuged, and the supernatant obtained was stored at 4°C for subsequent analysis.
Evaluation of Trace elements in saliva was performed by Microwave Plasma Atomic Emission Spectrometer (MP-AES):

Image courtesy: ICAR-Directorate of Cashew Research
MP-AES is a highly sensitive instrument for the detection of a wide range of elements down to sub ppb levels and is faster compared to conventional atomic absorption based instruments. Instead of flammable gases, MP-AES uses microwave energy to produce plasma for ionization of elements, using nitrogen extracted from ambient air. The excited electrons while returning to the ground state emits radiation characteristics to each element and the intensity of emission being proportional to the concentration of an element in the solution.
Results
|
Salivary Concentration |
Group |
N |
Mean |
SD |
Mean Difference |
95% Confidence Interval of the Difference |
t |
df |
p-value |
|
|
Lower |
Upper |
|||||||||
|
Zinc |
Caries Free |
30 |
18.92 |
2.28 |
12.88 |
11.68 |
14.07 |
21.55 |
58 |
<0.001* |
|
|
Caries Active |
30 |
6.04 |
2.35 |
|
|
|
|
|
|
|
Copper |
Caries Free |
30 |
4.58 |
2.37 |
-33.47 |
-39.92 |
-27.02 |
-10.38 |
58 |
<0.001* |
|
|
Caries Active |
30 |
38.05 |
17.50 |
|
|
|
|
|
|
Table 1:- Statistical Analysis Depicting the Level of Significance
Independent sample t test : *p<0.05 statistically Significant p>0.06 Non Significant,
The values obtained were statistically analyzed using the SPSS version 2.0 software. Caries free group showed a mean salivary zinc level of 18.92 microgram/L with a standard deviation of 2.28. Whereas caries active group showed a mean salivary zinc level of 6.04 microgram/L with a standard deviation of 2.35. The values showed a significant difference between the two groups.
Also, the caries-free group showed a mean salivary copper level of 4.58 microgram/L with a standard deviation of 2.37. Whereas caries active group showed a mean salivary copper level of 38.05 microgram/L with a standard deviation of 17.50. The values showed a significant difference between the two groups.
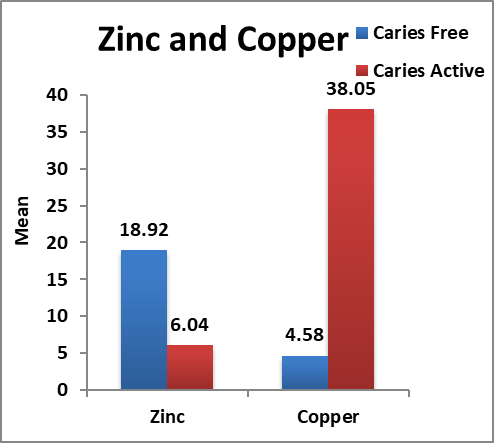
Graph 1: Depicts Graphical Representation of the Data
Discussion:
The salivary trace elements reflect the various metabolic activity and any change in these elements represents the change in the normal physiologic process. Qualitative and quantitative essay of these elements in saliva helps us evaluate their role in various oral conditions 21
The present study showed mean salivary zinc levels were significantly high in the caries-free group which might be attributed to the decreased dissolution of calcium in hydroxyapatite crystals due to its easy incorporation. Under cariogenic conditions, the levels in saliva will be low, less available zinc in plaque fluid, and on the tooth surface. This is following the study conducted by Sejdini M et al and contrary with a study conducted by Duggal et al and Mohammed et al in which authors mention there is no statistical correlation between salivary zinc levels and dental caries 22-24.
The study conducted on mice model by Bales and Freeland graves, Gregory et al and Fang et al were the mice were fed with a zinc-deficient diet, the incidence of caries was high 25-27. A similar study conducted by Zahir et al showed salivary zinc level significantly high in caries-free group and in comparison with group with multiple caries which is following our study 28 and the study conducted by Khrosh et al 29.
In the present study, salivary copper levels showed significant high level in caries active group compared to the caries-free group with is following the study conducted by Borella et al 30 which can be attributed to the dissolution of a minute amount of deposited copper into the saliva on tooth surface during the process of demineralization also may aid in various bacterial metabolism 31 Zahir S conducted a study which denied any significant correlation between caries active and high level of salivary copper levels which is following the study conducted by Duggal et. al 24, 26.
Therefore this study provides evidence of significantly high levels of zinc in the caries-free group and significantly high copper levels in caries active group. The study can be improvised by also correlating the dietary habits, geographic location, and water usage which would justify the source and provide brief detail supporting the evidence.
Acknowledgment:
ICAR-Directorate of Cashew Research, Darbe, Puttur for helping us with the equipment
Central research laboratory, KSHEMA
Prof. Krishna Bhat, Statistician, KSHEMA, Nitte deemed to be a university for helping us with the statistical analysis.
Funding: Self-funded.
References







