PREVALENCE OF CIVATTE BODIES IN ORAL LICHEN PLANUS AND ITS ASSOCIATION IN CUTANEOUS LESIONS
Aklesha Behera1, Reshma Poothakulath Krishnan2*, Deepak Pandiar2
1Coorg Institute of Dental Sciences, Virajpet, Karnataka, University in Aimangala, Virajpet, India.
2Department of Oral Pathology and Microbiology, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India. [email protected]
https://doi.org/10.51847/FlzOSDUsqI
ABSTRACT
Oral lichen planus is an autoimmune, chronic mucocutaneous lesion triggered by various etiological agents and affects the oral and genital mucous membranes, skin, nails, and scalp. It is relatively common and is associated with periods of exacerbation and remission. Civatte bodies are present in the basal layer of the oral epithelium in lichen planus. The study aimed to evaluate the prevalence of Civatte bodies in oral lichen planus and its association with cutaneous lesions. Slides of oral lichen planus were retrieved from the Department of Oral and Maxillofacial Pathology archives. Clinical details of the patients were collected, and the slides were evaluated for the presence of Civatte bodies. Evaluation was done, tabulations were made, and statistical analysis used SPSS version 20.0. The majority of the subjects were female patients. Of 32 cases, Civatte bodies were evident only in 15 cases (42.9%), and only one presented with a skin and oral lichen planus lesion. However, no civatte bodies were found. No association was not found between the quantification of Civatte bodies in oral lichen planus lesion and a probable manifestation of cutaneous lichen planus.
Key words: Oral lichen planus, Civatte bodies, Prevalence, Pathogenicity, Cutaneous lichen planus.
Introduction
Oral lichen planus is an autoimmune, chronic mucocutaneous lesion triggered by various etiological agents that affect oral and genital mucous membranes, skin, nails, and scalp. Hence, it is relatively common and associated with exacerbation and remission periods [1]. Lichen Planus is estimated to affect 0.5% to 2.0% of the general population. This disease has most often been reported in middle-aged patients with 30-60 years of age and is more prevalent among the female population than the males [2]. The word lichen planus comes from the Greek word 'Leichen,' which means tree moss, and 'planus' means flat [2, 3].
The histological features of oral lichen planus are basal cell degeneration, saw tooth rete pegs, a subepithelial band of lymphocytes, and Civatte bodies [4]. The presence of Civatte bodies is one of the important histopathological features of oral lichen planus. They are present in the basal layer of the oral epithelium. The Civatte bodies contain keratin intermediate filaments covered by immunoglobulins, mainly IgM. They are visible in routine histological sections and can be demonstrated by PAS stain. According to standard textbooks and many researchers, the presence of Civatte bodies can indicate interphase dermatitis [5].
The correlation between the presence of Civatte bodies in oral lichen planus and cutaneous lichen planus needs to be understood. It is well established that the presence of Civatte bodies in the epithelium denotes the presence of underlying dermatitis. Cutaneous lichen planus involves the flexor surfaces of the extremities and presents as small, itchy, violaceous papules in middle-aged adults. The aim of the study was to evaluate the prevalence of Civatte bodies in oral lichen planus and its association with cutaneous lesions.
Materials and Methods
Thirty-two (32) cases of oral lichen planus histological slides were retrieved from departmental archives, and evaluation was done for the presence of Civatte bodies in the light microscopy. Case details were taken, such as the age of the patient, gender of the patient, site of the lesion, clinical variant of the oral lichen planus, and associated cutaneous lichen planus if noted.
Civatte bodies scoring:
0: No civatte bodies found
1: 1-3 civatte bodies
2: 3-5 civatte bodies
3: > 5 civatte bodies
The data was entered in Microsoft Excel, and data interpretation and statistical interpretation were done using SPSS version 20.0
Results and Discussion
All the cases retrieved from the department archives were incisional biopsies (100%). Of 32 lichen planus cases, 17 were women (48.6%) and 15 were males (42.9%). The buccal mucosa was the most commonly presented site for lichen planus (82.9%). The maximum cases of lichen planus were observed between 40 to 45 years of age (20%), followed by 30 to 35 and 35 to 40 years (17.1%, 11.4%). Out of 32 cases, one was diagnosed as bullous lichen planus, 6 cases as erosive lichen planus, 7 as reticular lichen planus, and the remaining 18 cases were not provided with any clinical typing, hence diagnosed as lichen planus. Only in one case does the patient present with oral and cutaneous lichen planus.
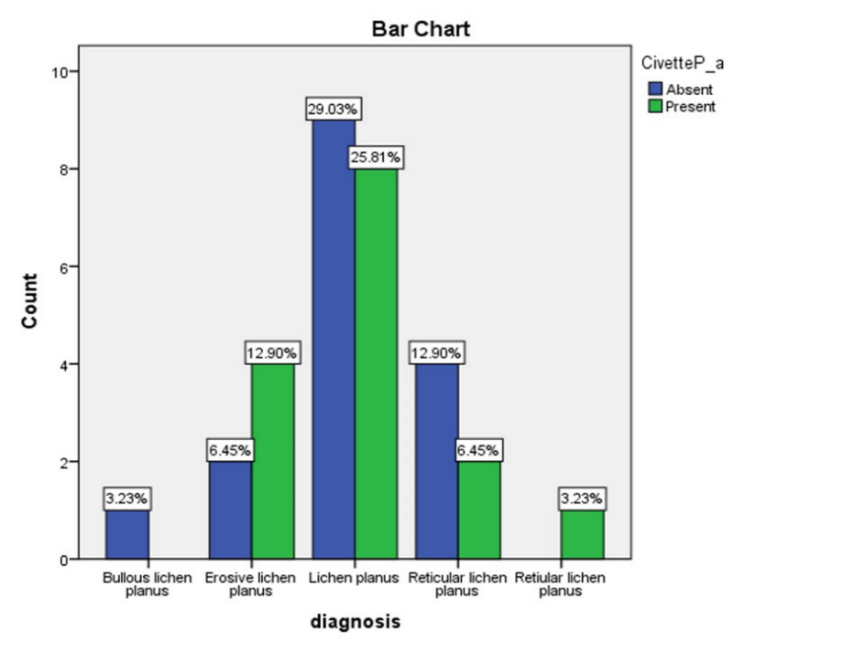
Of all the cases, only 15 showed the presence of civatte bodies (42.9%). A maximum of 2 Civatte bodies were observed in one slide, which was evident in 7 lichen planus cases (20%). All the 15 cases where civatte bodies were observed were that of oral lichen planus. Civatte bodies were not noted in the mucocutaneous lichen planus.
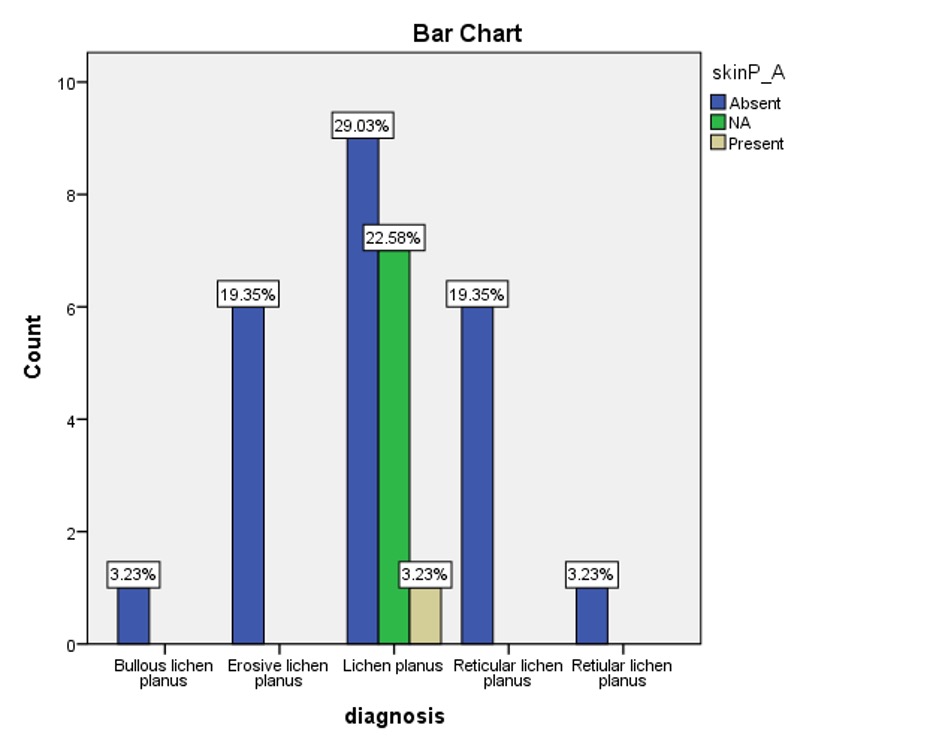
Association figures were made between the diagnosis and presence of civatte bodies. Figure 1 shows the association between the lichen planus types and civatte bodies' presence. Only 25.8% of the lichen planus presented with Civatte bodies, and erosive LP showed 12.9% of Civatte bodies. The association was found to be not significant. Another association between the diagnosis and the presence of skin LP was made (Figure 2). As there was only one skin LP, the association was not significant.
|
|
|
Figure 1. The bar graph shows the association between the clinical diagnosis of the lichen planus and the presence or absence of Civatte bodies. |
|
|
|
Figure 2. Graph shows an association between the clinical lichen planus types with any associated cutaneous planus. |
Lichen planus is an autoimmune, inflammatory disease that mostly affects skin and mucosal membranes [6]. Lichen planus in the skin appears to be presented as a pruritic, with plaques and papules affecting wrists, lower back, and ankles [7]. Oral lichen planus is a chronic mucocutaneous disorder of stratified squamous epithelium that affects oral mucosal membranes such as buccal mucosa gingiva with bilateral presentation of Wickham's striae [1]. It affects mostly women from the middle age group [8]. In our study, most participants were females and presented with bilateral presentation of lichen planus lesions on the buccal mucosa. This is following previous literatures [1, 9].
Civatte bodies are apoptotic/hyaline bodies found in lichen planus and other skin diseases [5, 9]. Raymond Sabouraud first discovered it in 1912 [10]. The pathogenesis of the disease is still undecipherable. Civatte bodies are somewhat understood to be immunologically altered cells in which basal keratinocytes present antigens with activation of CD4+ T helper, resulting in the release of cytokines, followed by cytotoxic reactions against the basal layer of epidermal cells. This action causes a rupture in the basal keratinocytes, leading to apoptosis and ultimately forming Civatte bodies [11].
Our study found that most of the Civatte bodies were found in older age groups. The reason is as age advances, the phagocytic property decreases, hence being unable to digest the Civatte bodies [12]. There is also a school of thought which states that the process of apoptosis does not take place in continuation. It has a definite intermittent process; hence, in many lichen planus incisional biopsy specimens, a pathologist finds locating the Civatte bodies difficult. This could be why we did not demonstrate Civatte bodies in our study slides. A study stated that oral lichen planus is more atrophic and shows greater apoptosis [13, 14].
It has been well documented that the presence of Civatte bodies indicates an interface dermatitis, hence making their presence pathognomonic in lesions such as Lichen Planus and Discoid Lupus Erythematosus, lichenoid reactions, systemic lupus erythematosus and so on lesions. In our study, however, the maximum number of Civatte bodies noted was 2, in which the only case presented with oral and cutaneous lichen planus did not show the presence of Civatte bodies in oral lichen planus slide during histopathological slide evaluation. A study stated that the skin lichen planus lesions show many Civatte bodies compared to other interface dermatitis. The Civatte bodies in the skin lichen planus are presented in groups of 5 to 10 cells [6].
Most literature states that the presence of Civatte bodies is a pathognomic indicator for lichen planus lesions, and it plays an important role in distinguishing from other interface dermatitis, such as lichen planus with lichenoid reactions [15, 16]. In lichenoid reactions, the Civatte bodies are placed in the more superficial layers of the epithelium. However, in lichen planus lesions, the Civatte bodies are located either subepithelial or on the basal layers [15]. The quantification of Civatte bodies in oral lichen planus leading to skin lichen planus is not mentioned in any literature. Many authors have noted that various immunological studies showed the deposition of IgM antibodies in Civatte bodies in various interphase dermatitis (cutaneous lesions), such as lichen planus lichenoid erythematosus. The quantity of Civatte bodies and IgM staining intensity is prominent in cutaneous lichen planus [15]. Even though quantification and staining intensity confirm that cutaneous lichen planus shows increased prevalence in Civatte bodies. Our study found no Civatte bodies in the oral lichen planus histological slide with cutaneous lichen planus presentation, thus bringing us to an inconclusive finding. Hence, no association was ruled out between the presence of Civatte bodies in oral lichen planus lesions and the probability of manifestation of cutaneous lichen planus in early or later stages.
Conclusion
It was concluded from our study that no association was found. Hence, we could not prove a hypothesis that an increased number of Civatte bodies in the oral lichen planus lesions leads to the formation or is an early indicator for the early onset of cutaneous lichen planus. A more thorough study has to be performed related to the topic with enough sample size, special stains, and immunohistochemistry markers for a detailed understanding of the topic.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None