Intentional replantation involves the purposeful extraction of a tooth, which is then reinserted back into its socket. It is considered one of the alternate options to be considered in the management of hopeless teeth presenting with advanced periodontal destruction in anterior teeth. Intentional replantation is generally opted for the management of endodontically reinfected teeth with good periodontal support and contraindicated in teeth with reduced periodontal support. The main advantage is that the inaccessible areas of the tooth surfaces can be easily visualized without causing damage to the adjacent periodontal tissues thereby promoting reconstruction of periradicular tissues. However, recent evolving studies have extended the method of intentional replantation for the periodontally hopeless tooth. This case report is about the management of a periodontally hopeless tooth with intentional replantation in the lower central incisor with simultaneous periapical surgery in the lateral incisor. This case has been followed up every three months for one year.
Introduction
The ultimate aim of periodontal therapy is to repair and regenerate the lost periodontium. From the biological and functional perspective, managing anterior teeth manifesting with advanced periodontal destruction is difficult and extraction may be required [1, 2].
Intentional replantation is the process of atraumatic extraction of teeth, and root end filling followed by repositioning into the socket [3, 4]. Some authors choose to utilize it as a last option to save a tooth for various reasons [5]. This is a simple, economical, and fast procedure with minimal postoperative discomfort [6]. The main advantage is that the inaccessible areas of the tooth surfaces can be easily visualized without causing damage to the adjacent periodontal tissues thereby promoting the reconstruction of periradicular tissues [7].
This case study aimed to showcase the clinical and radiological findings one year after intentionally replanting a periodontally affected hopeless tooth.
Case report
The systemically healthy 42 year-old female patient was referred to the Department of Periodontology for the management of mobile lower front teeth for the past 1 year. Intraoral examination in relation to the area of interest revealed gingiva was pale pink with melanin hyperpigmentation, rolled out margins with blunted interdental papilla, soft in consistency, loss of stippling, bleeding on probing with class IV recession in 31 and Class I recession in 32. Probing Pocket Depth of 5-6 mm and gingival recession of 5 mm were found in relation to 31 (Figure 1a). The width of the attached gingiva and Vestibular depth were adequate. Pathological migration with grade II mobility was seen in 31. Vitality test was performed by heat test and 31 and 32 were found to be non-vital.
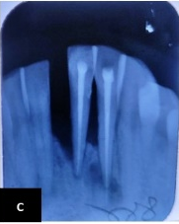
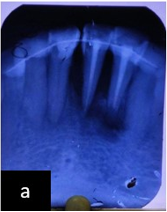
A radiographic examination done using Intraoral Periapical Radiographs revealed severe alveolar bone resorption reaching up to the apex of the mandibular left central incisor. An ill-defined periapical radiolucency of around 5 mm was noted in the left mandibular lateral incisor (Figure 1b). The patient was not willing for an extraction and wanted to save her natural tooth due to economic reasons. The treatment plan was determined to include phase I therapy and root canal treatment in teeth 31 and 32, based on the patient's needs and clinical condition (Figure 1c), followed by intentional replantation in 31 & apicectomy in 32.
|
|
|
|
a) |
|
|
|
|
|
b) |
c) |
|
Figure 1. a) Pre-operative photograph showing pathological migration and clinical attachment loss in 31. b) Intraoral Periapical Radiographs revealed severe alveolar bone resorption reaching up to the apex of the mandibular left central incisor and an ill-defined Periapical Radiolucency of around 5 mm noted in left mandibular lateral incisor. c) Post-RCT in 31 and 32 |
|
Surgical procedure
The Surgery was performed under an aseptic protocol. Local Anaesthesia was administered as left Inferior Alveolar Nerve Block and right Mental nerve block using Lidocaine 2% (Figure 2a). Sulcular and Interdental incisions were placed from the distal aspect of 33 to the distal aspect of 43 (Figure 2b) with a vertical releasing incision at the distofacial papilla of the canine to reflect a rectangular flap on the labial side (Figure 2c).
In relation to 32, Osteotomy was carried out at the predetermined area (from the IOPA) using a straight fissure carbide bur. Apical curettage was done using Curettes, 3 mm root-end resection and retrograde root-end filling was done using Glass Ionomer Cement (Figure 2d).
In relation to 31, an atraumatic tooth extraction was performed, followed by meticulous root planing to remove any necrotic cementum and granulation tissue. Subsequently, the removed tooth was submerged in normal saline (Figure 2e). The tooth socket is prepared for replantation by using a sequence of implant drills D2 and D3. The removed tooth was inserted into the socket and secured with an extra coronal splint using 26-gauge wire from tooth 33 to tooth 43 (Figure 2f). Flaps are then approximated using simple interrupted sutures using non-resorbable suture 3-0 Black silk (Figure 2g). Acrylic cap splints were fabricated and placed in the lower anterior region for apicocoronal stabilization (Figure 2h). Antibiotics and analgesics were prescribed for 5 days.
|
|
|
|
a) |
b) |
|
|
|
|
c) |
d) |
|
|
|
|
e) |
f) |
|
|
|
|
g) |
h) |
|
Figure 2. a) Pre-operative view. b) Sulcular and Interdental incisions were placed from distal aspect of 33 to distal aspect of 43 with vertical releasing incision at distofacial papilla of canine. c) rectangular flap reflected on labial side. d) Apicectomy in 32. e) Atraumatic extraction of 31. f) Tooth is replanted into extracted socket and stabilized using extracoronal splinting. g) Acrylic splint. h) Periodontal dressing placed. |
|
Post-operative review was done in 10 days. The acrylic splint was removed and teeth were stabilized using composite stops. Suture removal was carried out. Post-operative review at 6 weeks revealed satisfactory healing (Figure 3a). Extracoronal splint was replaced with intra-coronal splinting using braided ligature wire and composite (Figure 3b).
|
|
|
|
a) |
b) |
|
Figure 3. a) 6 weeks post-operative clinical photograph. b) Intra-coronal splinting |
|
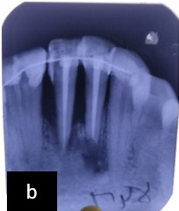
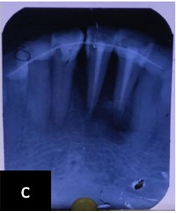
Post-operative re-evaluation at 3 months revealed slight haziness surrounding 31 suggestive of possible bone formation radiographically (Figure 4a) and reduction in PPD and BOP clinically (Figure 5a). Re-evaluation at 6 months and 12 months revealed increased radio density surrounding 31 radiographically (Figures 4b and 4c) and further reduction in PPD and patient acceptance clinically (Figures 5b and 5c).
|
|
|
|
a) |
b) |
|
|
|
|
c) |
|
|
Figure 4. a) IOPA at 3 months follow-up. b) IOPA at 6 months follow-up. c) IOPA at 1 year follow-up |
|
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
Figure 5. a) Clinical photograph at 3 months. b) Clinical photograph at 6 months. c) Clinical photograph at 1 year |
Results and Discussion
Prognosis has been defined by Carranza as the probable course, duration, and outcome of a disease and the likelihood of its response to treatment, based on the general knowledge of the pathogenesis of the disease and the presence of risk factors. It has been classified as follows [8]:
Good prognosis: Control of Etiological factors and adequate periodontal support,
Fair prognosis: 25% attachment loss and/or class I furcation,
Poor prognosis: 50% attachment loss, Class II furcation,
Questionable prognosis: >50 attachment loss, class III furcation, Poor crown root ratio, >2+ mobility
Hopeless prognosis: Inadequate attachment to maintain health, comfort and function.
In this case, the mandibular left central incisor is associated with bone loss extending to the apex of the tooth with Grade II mobility. The tooth is said to have a hopeless prognosis since it cannot maintain health, comfort and function. The ideal treatment is extraction of the tooth followed by dental implants. However, the patient was not willing for extraction and demanded to save her natural tooth so we decided to take up Intentional Replantation, the last resort option as the treatment plan.
Research findings indicated a 25% reduction in bone volume in the first year and a 40-60% drop in breadth during the first 3 years after tooth loss. Intentional replantation application helped prevent post-extraction alveolar crest height and breadth decrease [9].
Demiralp et al. studied the clinical and radiographic results of intentional replantation in 15 periodontally hopeless teeth. At the end of six months, the author demonstrated reduction in PPD clinically and no root resorption or ankylosis was observed radiographically [1]. Intentional replantation was suggested as an alternative approach to extraction when no other treatments could be considered [10].
If the extra-oral dry time exceeds two hours, there is a 95% probability of external resorption and non-functional scar [11], as described by Anderson [12]. Dryden et al. 1994 recommended that the time lapse between extraction and replantation treatments should not surpass 15 minutes [13]. All replantation operations were finished in around 30 minutes in this case report.
Nagappa et al. (2013) did intentional replantation of the maxillary central incisor in 2 cases with moderate probing depth of 6 mm & grade II mobility without using a root conditioning agent and attempted regeneration 3 months following intentional replantation and gained improved clinical outcome and radiographic bone fill [14]. Sen et al. (2020) reported case series on intentional replantation with better clinical and radiographic outcomes in 6-months follow-up without attempting bone grafts & PRF [15].
In this case, since we have planned for flap reflection for Intentional replantation in the mandibular left central incisor, the periapical lesion in the mandibular lateral incisor is treated simultaneously. This is the first case report showing simultaneous periodontal endodontic surgery treated concurrently.
This case has been followed up for 1 year at a monthly interval and showed a significant reduction in probing pocket depth and bleeding on probing and a slight increase in clinical attachment loss probably due to shrinkage of gingival epithelium. Radiographically, the bone loss % is calculated by the formula given by Schulte et al. [16] and found to be pre-operatively 69.2%, 3-month post-operatively 64.1%, 6-month post-operatively 53.8% and 1 year post-operatively 48.5%. This revealed a total bone gain of around 20.7%. Patient satisfaction and patient compliance were found to be good. This brings forth that the procedure was successful in this patient.
Conclusion
The primary objective of dentistry is to maintain a tooth in the mouth for as long as feasible. Intentional re-implantation helps preserve the integrity of natural teeth. It enhances the appearance and functionality of the smile by preserving natural teeth that are deemed to have a poor outlook.
In the present case, a favorable clinical and radiographic outcome was reached, yet further long-term clinical, radiographic and histological evaluation is required to validate this outcome.
Acknowledgement: None
Conflict of interest: None
Financial support: None
Ethics statement: None