
Fibrolipoma of Buccal Mucosa: An Unusual Case
Varsha VK1*, Vasant Kattimani2, Mamta S Kamat 3
1 Reader, Department of Oral Pathology and Microbiology,Rajarajeswari Dental College & Hospital, Bangalore 560075.
2Specialist, Oral and Maxillofacial Surgery, District Hospital, Dharwad 580001.
3Associate Professor,Department of Oral Pathology and Microbiology,Bharati Vidyapeeth (Deemed to be University) Dental College and Hospital, Sangli, 416416.
ABSTRACT
Fibrolipoma is one of the infrequent variants of Lipoma characterized by distinctive features with both mature adipose cells and broad bands of intense fibrous connective tissue. It may be present at birth which is caused by an endocrinal imbalance, originate via the disintegration of a fibromatous tumor, arises from the maturation of lipoblastomatosis, and also due to repeated mild trauma which triggers the proliferation of fatty tissue. It has a diverse clinicopathologic and biologic entity with amplified growth potential but with a low recurrence rate. Here we report details of a case of Fibrolipoma in a 53-year-old male occurring in the right buccal mucosa extending from 46 to 48 regions.
Key words: Buccal mucosa, Fibrolipoma, Lipoma.
Introduction
In low and middle income countries, cervical cancer 1 is considered one of the common cause of cancer related-death 2-4. Neoplasia is an amateurishly understood phenomenon which is defined as an unusual mass of tissue, the growth of which can go beyond and is uncoordinated with that of the normal tissues and persists in the same excessive manner after the termination of the stimuli that evoked the change. A discrete mass of tissue can be either benign or malignant.5
The lipoma is one such benign tumor of adipocytes. It represents the most frequent mesenchymal neoplasm, and the majority of cases occur on the trunk and proximal portions of the extremities; on the other hand, lipomas of the oral and maxillofacial region are rare. Their overall prevalence in the oral cavity is thought to be less than 4.4 % of all benign oral mesenchymal neoplasms.6 It does not have any gender predilection but commonly is seen in adults above 30 years of age.5 Although oral lipoma is commonly asymptomatic, it may interfere with speech and mastication.7 Oral lipomas can be seen in various anatomic sites such as major salivary glands, buccal mucosa, lip, tongue, palate, vestibule, and the floor of mouth.8 Based on their histological features lipomas can be categorized as classic lipomas or its variants. Surgical removal is the foremost choice of treatment for lipoma. The complete resection should be done to avoid the recurrence.5 Here we describe a case of Fibrolipoma in a 53-year-old male occurring in the right buccal mucosa extending from 46 to 48 regions.
Case Report:
A 53-year-old male patient reported at the Department of oral and maxillofacial surgery, General hospital, Kalghatgi, with a chief complaint of a painless swelling on the right side of the cheek for five years. The swelling was initially small, and a gradual increase in size was observed. His past family, medical, and dental history was not significant. Extra orally no abnormality was detected. Intraoral examination revealed Pedunculated, nodular, well-defined, smooth-surfaced swelling measuring about 3.5 × 2.5 cm on right buccal mucosa distal to 47 regions. The mucosa covering the swelling was normal [Figure 1]. On palpation; it was non-tender and soft in the consistency.
With a provisional diagnosis of lipoma, the lesion was excised under local anesthesia, hemostasis achieved, BBS suture given [Figure 2], and the excised specimen [Figure 3] was subjected for histopathological examination. Histopathological examination of excised specimens revealed a circumscribed lesion with parakeratinised stratified squamous epithelium surface epithelium and dense mature connective tissue stroma.
The stroma comprised of a lobular arrangement of mature adipocytes along with interspersed numerous collagen fiber bundles [Figure 4]. The adipocytes were large round to ovoid cells with clear cytoplasm and eccentric nuclei compressed against the cytoplasmic membrane. By considering the above and clinical features a final diagnosis of Fibrolipoma was rendered.
Discussion:
Oral lipoma first described by Roux in 1848 was referred to as yellowish epulis. This benign slow-growing neoplasm is metabolically varied from normal fat cells even though they are histologically similar.5Trauma and chronic irritation have also been mentioned as triggers for the proliferation of fatty tissue into a benign tumor. Hereditary and chromosomal abnormalities including rearrangements of 12q, 13q, and 6p chromosomes have also been mentioned in a few cases.9 Intraoral lipomas can be morphologically classified as diffuse, superficial and encapsulated form. Numerous head and neck lipomas are noticed in various conditions such as neurofibromatosis, Gardner syndrome, encepalocraniocutaneous lipomatosis, multiple familial lipomatosis and Proteus syndrome.5
Radiographically it has a distinctive radiographic appearance. On computed tomography scan it demonstrates a high density from 83 to 143 Hamsfield units with well or poorly defined margins depending on the capsule. Ultrasonography illustrates a lesion that is round or elliptical in shape with an intact or mostly intact capsule. Most lipomas are hypoechoic with ecogenic lines or spots.10
Histopathologically lipomas can be categorized as: (i) classical lipoma; (ii) lipoma variants, such as Fibrolipoma, angiolipoma, chondroid lipoma, myelolipoma and spindle cell/pleomorphic lipoma, all with specific clinical and histological features; (iii) hamartomatous lesions; (iv) diffuse lipomatous proliferation; and (v) hibernoma. In the present case, histopathological features were suggestive of Fibrolipoma.11
Classic lipoma cases are most commonly seen followed by Fibrolipoma. It is histopathologically characterized by a significant fibrous component intermixed with lobules of adipose tissue. The etiopathogenesis remains unknown. Various studies have suggested that it may be a congenital lesion caused by an endocrinal imbalance, arises via the degeneration of a fibromatous tumor, arises from the maturation of lipoblastomatosis and also can arise because of repeated mild trauma which triggers the proliferation of fatty tissue 12 The proliferative activity in Fibrolipoma is enormous; a precise diagnosis is very important which can be done by histopathological examination of the lesion to prevent over or under treatment.13
Treatment modality for intraoral Lipoma is complete surgical excision. No recurrence has been described after local excision. Smaller lipomas can also be medically managed by injecting steroid injections that will result in fat atrophy and shrinkage of the tumor. Repeated monthly injections of 1:1 combination of lidocaine and triamcinolone acetonide into the innermost area of the tumor can regress the lesion. 14
References
Corresponding Author
Dr.Varsha VK,
Reader, Department of Oral Pathology and Microbiology, Rajarajeswari Dental College and Hospital, # 14 Ramohalli Cross, Kumbalgodu, Bangalore 560074India.
Email: [email protected]
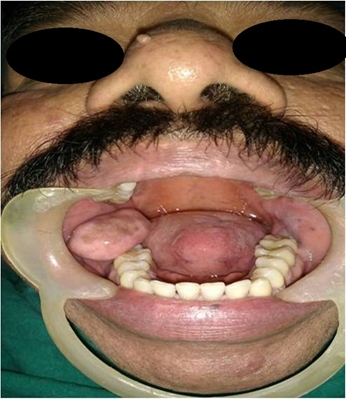
Figure 1: A nodular mass in the right mandibular buccal vestibule opposite to the premolars and molar region.
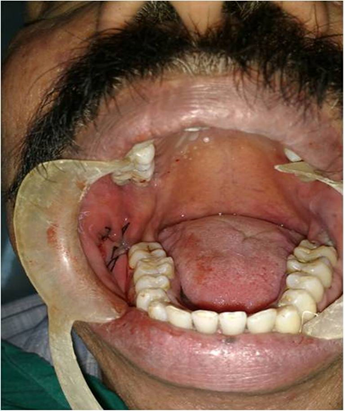
Figure 2: Postoperative photograph.

Figure 3: Excisional specimen.
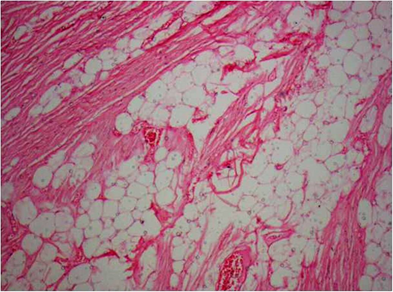
Figure 4: Photomicrograph showing lobular arrangement of mature adipocytes along with interspersed numerous collagen fiber bundles (40x).

