
Assessment Of Dental Anxiety Among The Adolescent Patients Visiting The Private University Undergraduate Dental Clinics In Riyadh City, Saudi Arabia
Dalal Rasheed AlAssadi 1*, Nasser Ibrahim Alduhaimi1, Farah Ghalib AlSaadoun1, Wsayef Hammad Almarzuqi2, Mona Ahmed Alenezi1, Faisal Mansour Binhayyan3, Sunil Babu Kotha4
1 Dental Intern, College of Dentistry, Riyadh Elm University, Riyadh, Saudi Arabia
2 Dental Intern, AlMustaqbal University, Al Qassim, Saudi Arabia
3 Demonstrator, Department of Preventive Dentistry, Prince Sattam University, Al-Kharj, Saudi Arabia
4 4 Faculty Department of Preventive Dentistry, College of Dentistry, Riyadh Elm University, Riyadh, Saudi Arabia.
ABSTRACT
Background: Dental anxiety among children and adolescence is correlated with a sequence of uncooperative or troubling behaviors. The purpose of this study was to assess the prevalence and factors affecting dental anxiety among adolescent patients seeking dental treatment by undergraduate dental students in the college of dentistry, Riyadh Elm University, Riyadh, Saudi Arabia.
Materials and Methods: A convenient sampling methodology was employed to select 777 adolescent patients seeking care from undergraduate dental students. A structured, close-ended Arabic version of the modified dental anxiety scale was self-reported by the patients in the waiting area of the dental clinics. Descriptive statistics, Mann-Whitney, and Kruskal-Wallis tests were applied to compare the dental anxiety scores between groups.
Results: The age of the participant ranged from 13-19 years. The majority of the study participants were in the moderate (39.4%) category of dental anxiety, followed by mild (32.6%), severe (14.4%), and high (13.6%). Female patients showed a significantly higher score on the Modified Dental Anxiety Scale compared to the males (13.46±0.21 vs. 10.98±0.27, p<0.001). Patients having university education showed a higher mean score (13.29±0.32), followed by middle school (12.75±.36), high school (12.11 ±.25), and elementary school (11.29±1.72). However, the educational level did not show any significant effect on dental anxiety (p=0.053).
Conclusion: The majority of adolescent patients treated by dental students showed moderate degrees of dental anxiety. However, dental phobia was found in 14.4% of adolescents. Females demonstrated a higher degree of dental anxiety than males. The level of education did not display any impact on dental anxiety among adolescents in this study.
Key words: Dental anxiety, modified dental anxiety scale, adolescent patients, dental students
Introduction
Dental fear typically applies to natural adverse emotional responses to particular threatening stimuli due to dental treatment-related conditions, whereas dental anxiety is an excessive and unreasonable harmful emotional condition encountered by dental patients.1-4 Dental fear typically applies to natural adverse emotional responses to particular threatening stimuli resulting in dental treatment-related conditions, whereas dental anxiety is an excessive and undue harmful emotional condition encountered by dental patients. These psychological conditions compose of the apprehension that something bad is about to occur anytime during dental care. Dental fear and dental anxiety are sometimes used indistinctly in literature but reflect separate increments of the same psychological condition.5 Extreme dental anxiety, impacting 10% to 20% of the adult population, 6,7 significantly affects dental attendance, dental care, and, eventually, oral health.8
Individuals with elevated dental anxiety levels frequently find themselves in a self-perpetuating cycle of fear, refusing routine dental care, pursuing help only when they are in pain, and having extensive dental needs for which invasive procedures are considered the most appropriate. People trapped in this cycle usually show poor oral health in addition to anxiety.9
Since dental treatment is ignored, it is not shocking that individuals with higher dental anxiety frequently have serious oral health issues. Avoidance of dental treatment and anticipatory distress have been correlated with a more significant number of lost teeth.10,11 It has been observed that the people with elevated dental anxiety have slightly higher ratings on the Oral Health Effect Profile, with feelings of self-consciousness and loss of life satisfaction more frequently nervous.12
Moreover, individuals with a high anxiety level were twice as likely to score low on oral health-related quality of life.13 Ultimately, people with elevated dental anxiety report significant impacts on their social, behavioral, and health functioning, including changes in oral health and inadequate sleep.14 However, anxiety among children and adolescence is correlated with a sequence of uncooperative or troubling behaviours.15, 16
This dental-associated fear with differing degrees of intensity is a phenomenon identified in studies performed in various regions of Saudi Arabia. A study conducted in Riyadh city reported that 29 % of adolescent females had a high degree of dental fear and anxiety.17The dental anxiety level in Saudi patients was comparatively higher (27.5 %) than in other studies with higher DA registered in Jeddah (31.9%) compared to Dammam (22.7 %).
Various measures have been designed to assess several facets of dental anxiety, such as the Corah Dental Anxiety Scale, the Modified Dental Anxiety Scale, the Southard Dental Anxiety Inventory Short Form, and the Dental Anxiety Survey.18 The dental anxiety scale, developed by the American Psychologist Norman Corah (Corah's Dental Anxiety Scale) in 1968, was the most widely used. Whereas, Modified dental anxiety scale is an enhanced version of the original Corah's dental anxiety scale, is commonly used, and is considered more useful in the clinical environment for the screening and diagnosing patients with dental anxiety.19 The other advantage of the modified dental anxiety scale include its reliability, validity, and capacity to be translated into different languages.20-22
Whenever dental students/clinicians treat patients with dental anxiety, they are invariably subjected to high stress, 23 with longer time-consuming treatments, high costs, and other problems encountered during their dental practice.24 This associated dental fear needs to be identified and quantified to categorize the patients and provide appropriate measures to alleviate their dental anxiety. Many adolescent patients visit dental clinics of dentistry, Riyadh Elm University, who were treated by the undergraduate dental students. However, limited data is currently available on dental anxiety among adolescents seeking dental care by undergraduate dental students. Hence this study aimed to assess the prevalence and factors affecting dental anxiety and phobia among adolescent patients seeking dental treatment by undergraduate dental students in the college of dentistry, Riyadh Elm University, Riyadh, Saudi Arabia.
Materials and Methods
Study design: A cross-sectional survey was conducted from August – December 2019 to assess dental anxiety among adolescent dental patients.
Ethical approval: The study proposal was registered in the research center of Riyadh Elm University (FRP/2019/65), and the ethical approval for the study was obtained (RC/IRB/2019/234). Informed consent to participate in the study was obtained from the patients or their accompanied parents.
Study participants: Adolescent dental patients aged between 13-19 years, receiving treatment from the dental students, mentally and physically stable to answer the Arabic version of the questionnaire were included in the study. Dental Patients who were not within the defined age-limits and uneducated, and cannot read and write were excluded from the study.
Sample size: A convenient sampling technique was applied to select adolescent dental patients attending clinics in dentistry colleges, Riyadh Elm University. A recommended sample size of 377 study participants was calculated by considering the margin of error (5%), the confidence level of (95%), and the distribution of a response rate of (50%). However, to improve the study's power, a final sample of 777 were included in the study. Sample size calculation was performed by using the Raosoft online sample size calculator.
Study instrument: A structured, close-ended, and self-administered questionnaire consisting of demographic information (age, gender, and education) and a modified dental anxiety scale was distributed to the adolescent patients. The questionnaire consisted of demographic information (age, gender, and education) and an Arabic version of the modified dental anxiety scale with 5 items (feeling towards treatment tomorrow, feeling towards waiting for the treatment, feeling towards tooth drilling, feeling toward scaling and polishing, and feeling toward local anesthetic injection). The questionnaire items were rated on a 5-point scale ranging from not anxious to extremely anxious, reflecting the Modified dental anxiety scale responses format, i.e., 1 = not anxious, 2 = slightly anxious 3 = fairly anxious4 = very anxious 5 = extremely anxious.20,25 A total score of the Modified dental anxiety scale was calculated by summing of all five items. It ranged from 5 to 25, and the final score was categorized as 5–9 mild anxiety, 10–15 moderate anxiety, 16–18 high anxiety, and 19–25 severe anxiety (phobia)
Questionnaire administration: A paper-based and electronic version of the questionnaire was distributed to the adolescent patients in the clinics' waiting area. It took less than 3-5 minutes to answer the questions. All the questionnaires were collected, responses were coded and entered into the excel spreadsheet.
Statistical analysis
All the data from the excel spreadsheet is transferred into the Statistical Package for Social Science (IBM SPSS statistics for windows, version 22.0. Armonk, NY: IBM Corp: USA) for the statistical analysis. Descriptive statistics of frequency distribution, percentages, mean and standard deviation were calculated for the study variables. The questionnaire responses of all the five items were calculated to obtain the overall anxiety score. Further, questionnaire items were scored as not anxious=0, all other responses (slightly anxious, fairly anxious, very anxious, and extremely anxious) were scored as 1. The relationship between the questionnaire items with different gender and educational levels was assessed using the Chi-square test. Data showed non-normal distributions. Hence mean Modified Dental Anxiety score between genders was compared by using the Mann-Whitney U test, and the Kruskal-Wallis test was applied to compare the mean score among different educational levels. A value of p<0.05 was considered significant for all the statistical purposes.
Results
Out of 800 total questionnaires distributed, 777 questionnaires were received by giving a response rate of 97.12%.
|
Characteristics |
n |
% |
|
|
Gender |
Male |
255 |
32.8% |
|
Female |
522 |
67.2% |
|
|
Total |
777 |
100.0% |
|
|
Education |
Elementary school |
7 |
0.9% |
|
Middle school |
154 |
19.8% |
|
|
High school |
344 |
44.3% |
|
|
University |
272 |
35.0% |
|
|
Total |
777 |
100.0% |
|
Table 1: Characteristics of the study participants
A total of 777 dental patients visiting out-patient undergraduate dental clinics of dentistry college, Riyadh Elm University, participated in the study. The majority of the study participants were female, 522(67.2%) having a high school level of education, 344 (44.3%). The characteristics of the study participants are described in Table 1.
|
Items |
NA |
SA |
FA |
VA |
EA |
|
Treatment tomorrow |
256 (32.9%) |
274 (35.3%) |
139(17.9%) |
73(9.4%) |
35 (4.5%) |
|
Waiting room |
251(32.3%) |
249(32.0%) |
131(16.9%) |
92(11.8%) |
54 (6.9%) |
|
Tooth drilled |
97(12.5%) |
199(25.6%) |
191(24.6%) |
151(19.4%) |
139 (17.9%) |
|
Teeth scaled and polished |
369(47.5%) |
228 (29.3%) |
106(13.6%) |
44(5.7%) |
30(3.9%) |
|
Local anesthetic injection |
104(13.4%) |
175(22.5%) |
143 (18.4%) |
139(17.9%) |
216(27.8%) |
Table 2: Distribution of the questionnaire responses
Most patients felt slightly anxious about visiting the dentist for dental treatment tomorrow 274 (35.3%), and when they were about to have a tooth drilled 199(25.6%). While waiting in a room for the treatment, 251(32.3%) and having teeth scaled and polished 369(47.5%), patients did not show any anxiety. However, 216(27.8%) patients felt extremely anxious while having a local anesthetic injection (Table 2).
|
Items |
Gender |
Educational level |
|||||||||||
|
Male |
Female |
Elementary |
Middle |
High school |
University |
||||||||
|
n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
||
|
Treatment tomorrow |
No anxiety |
116 |
45.5 |
140 |
26.8 |
3 |
42.9 |
50 |
32.5 |
119 |
34.6 |
84 |
30.9 |
|
Anxiety |
139 |
54.5 |
382 |
73.2 |
4 |
57.1 |
104 |
67.5 |
225 |
65.4 |
188 |
69.1 |
|
|
P |
<0.001 |
0.705 |
|||||||||||
|
Waiting room |
No anxiety |
102 |
40.0 |
149 |
28.5 |
2 |
28.6 |
45 |
29.2 |
113 |
32.8 |
91 |
33.5 |
|
Anxiety |
153 |
60.0 |
373 |
71.5 |
5 |
71.4 |
109 |
70.8 |
231 |
67.2 |
181 |
66.5 |
|
|
P |
0.001 |
0.834 |
|||||||||||
|
Tooth drilled |
No anxiety |
52 |
20.4 |
45 |
8.6 |
2 |
28.6 |
15 |
9.7 |
38 |
11.0 |
42 |
15.4 |
|
Anxiety |
203 |
79.6 |
477 |
91.4 |
5 |
71.4 |
139 |
90.3 |
306 |
89.0 |
230 |
84.6 |
|
|
P |
<0.001 |
|
0.109 |
||||||||||
|
Teeth scaled and polished |
No anxiety |
148 |
58.0 |
221 |
42.3 |
4 |
57.1 |
90 |
58.4 |
172 |
50.0 |
103 |
37.9 |
|
Anxiety |
107 |
42.0 |
301 |
57.7 |
3 |
42.9 |
64 |
41.6 |
172 |
50.0 |
169 |
62.1 |
|
|
P |
<0.001 |
<0.001 |
|||||||||||
|
Local anesthetic injection |
No anxiety |
53 |
20.8 |
51 |
9.8 |
3 |
42.9 |
13 |
8.4 |
52 |
15.1 |
36 |
13.2 |
|
Anxiety |
202 |
79.2 |
471 |
90.2 |
4 |
57.1 |
141 |
91.6 |
292 |
84.9 |
236 |
86.8 |
|
|
P |
<0.001 |
0.029 |
|||||||||||
Table 3: Dental anxiety among different gender and education levels
Dental anxiety among different genders and education levels are shown in Table 3. The majority of the females than males felt anxious about visiting the dentist for treatment tomorrow [382(73.2%) vs. 139 (54.5%), p<0.001], waiting in a room for the treatment [373 (71.5%) vs. 153 (60.0%), p=0.001], about the tooth to be drilled [477 (91.4%) vs. 203(79.6%), p<0.001], about the teeth scaled and polished [477 (91.4%) vs. 203 (79.6%), p<0.001], and about getting local anesthetic injection [471(90.2%) vs. 202 (79.2%), p<0.001]. Similarly, the educational level of the study participants showed significant differences with regards to the dental anxiety while teeth scaled and polished (p<0.001) and about to have a local anesthetic injection (p=0.029).

Figure 1: Distribution of Modified Dental anxiety scores
The distribution of the modified dental anxiety scores is shown in figure 1. The majority of the study participants were in the moderate (39.4%) category of dental anxiety, followed by mild (32.6%), severe (14.4%), and high (13.6%).
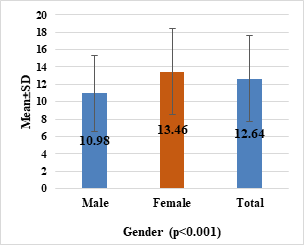
Figure 2: Comparison of mean Modified Dental Anxiety score between genders
Female patients showed a significantly higher score on the Modified Dental Anxiety Scale compared to the males (13.46±0.21 vs. 10.98±0.27, p<0.001) (Figure 2)
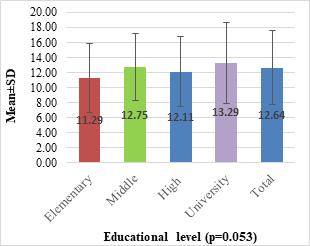
Figure 3: Comparison of mean score among different educational levels
Patients having university education showed a higher mean score (13.29±0.32), followed by middle school (12.75±.36), high school (12.11 ±.25), and elementary school (11.29±1.72). However, a comparison of the mean anxiety score did not yield any significant difference across the study participants' different education levels (p=0.053) (Figure 3).
Discussion
This study assessed the prevalence of dental anxiety levels in a sample of adolescent dental patients receiving dental care in private university dental clinics in Riyadh City, Saudi Arabia. An Arabic version of the modified dental anxiety scale with proven validity and reliability was utilized in this study. The prevalence of dental anxiety (score ≥ 10) was high (67.4%) among adolescent dental patients. Studies conducted from Saudi Arabia have reported a prevalence of dental anxiety varying from 27.5%-54.4%.17, 25 simultaneously, the prevalence of severe dental anxiety or dental phobia (score ≥ 19) among the adolescent study participants was found to be14.4%. Our study finding is lower than that reported by Al-Madi and Abdellatif 17 among female adolescents in Saudi Arabia, wherein the prevalence of high dental anxiety was observed in 29% of the study participants. However, the prevalence of high dental anxiety varied in Sweden (5.4%), 26 Malaysia (3.5%) 27 and India (3%).21
This reported disparity in the prevalence of severe dental anxiety may be clarified by differences in subject age groups in these studies, where participants were drawn from patients visiting dental clinics of various settings.28 In our study, only adolescent dental patients aged between 13-19 years receiving dental treatment from the undergraduate dental students were assessed for their dental anxiety levels. Additionally, choosing a cut-off point to categorize dental anxiety levels can cause a difference in reporting dental anxiety prevalence.28In this study a modified dental anxiety scale is divided into four categorize to report dental anxiety levels. Our study reported that many study participants were in moderate to mild categorize of dental anxiety scale. Another likely cause for a high level of anxiety observed in our study could be the high proportion of adolescent patients who are typically apprehensive.29
The current literature suggests that females have a lower threshold of pain tolerance and typically experience higher anxiety levels.30, 31Similar findings were observed in our study, which reported significantly higher dental anxiety levels among females than males. Similar results were reported in previous studies carried in different parts of the world. 21, 25, 28, 32 This finding could be because females tend to experience more negative emotional states (neuroticism) than males in whom anxiety is positively associated with emotional states.33, 34
Although the mean dental anxiety scores varied across different educational levels, there was an increase in the dental anxiety scores with increasing education years. However, our results indicated that educational level had no significant effect on dental anxiety of the adolescents receiving care from dental students. This finding is in line with the study reported by Arsalan et al. 35 in which no significant difference in the dental anxiety score was observed across various educational levels.
We have some limitations in this study. The data in our study focused on self-reporting, and their responses could be susceptible to prejudice. The study was conducted in a private dental university set-up. Hence, it may be difficult to apply to other dental settings, such as government schools or private dental clinics. The adolescent subjects' dental fear and anxiety were assessed, limiting the application of findings to other age groups. The cut-off points of modified dental anxiety scales considered in this study may be different from other studies. Only dental adolescent patients seeking care from dental students were considered in this study. Thus limiting the generalizability of the results of this study. Further large scale studies involving important age groups and various sociodemographic factors should be considered.
Conclusions
The majority of adolescent patients treated by dental students at a private dental university showed moderate degrees of dental anxiety. Relatively large dental phobic (14.4%) adolescents have also been documented relative to other research. Females have a higher degree of dental anxiety than males, hence they should be thoroughly screened to develop dental anxiety prevention techniques. However, the level of education did not display any effect on dental anxiety among adolescents in this study.
References
Corresponding Author
Dalal R AlAssadi
Dental Intern, College of Dentistry, Riyadh Elm University, P.O. Box 84891, Riyadh 11681, Kingdom of Saudi Arabia.

